1 Department of Medical Epidemiology and Biostatistics Karolinska Institutet Stockholm Sweden.
2 Novartis Pharma AG Zurich Switzerland.
J Am Heart Assoc. 2019 Jun 4;8(11):e012638. doi: 10.1161/JAHA.119.012638. Epub 2019 May 29.
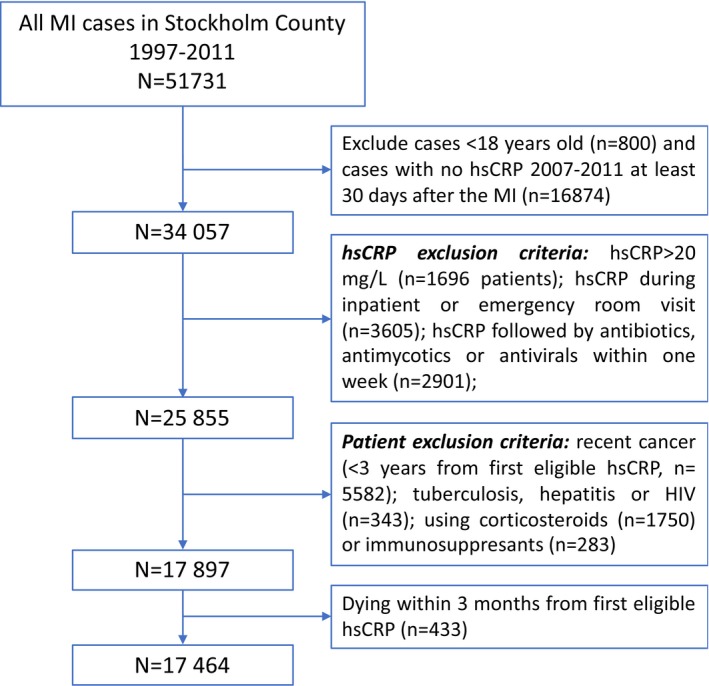
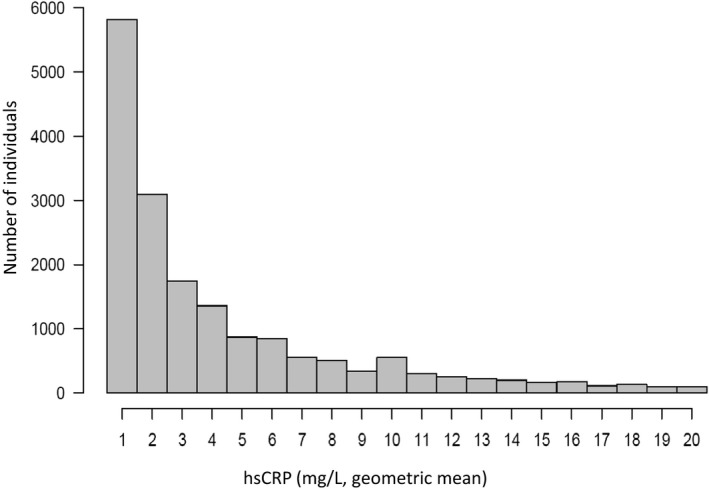
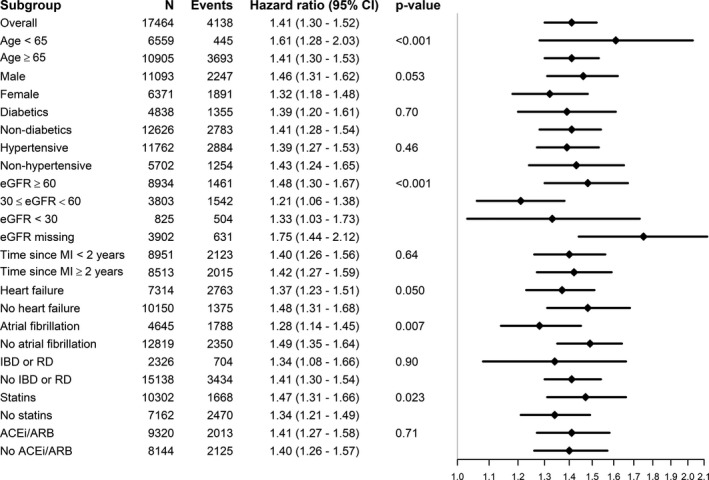
Background Beyond the controlled setting of trials, scarce information exists on the burden, predictors, and outcomes associated with elevated hs CRP (high-sensitivity C-reactive protein) in "real-world" patients with myocardial infarction ( MI ). Methods and Results We included all-coming MI survivors undergoing hs CRP testing >30 days after an MI during routine health care in Stockholm, Sweden (2006-2011). hs CRP tests measured during hospitalization/emergency department visits, followed by antibiotics or indicative of acute illness, were excluded, together with patients with ongoing/recent cancer, chronic infections, or immunosuppression. Inflammation was defined over a 3-month baseline window and associated with subsequent death and major adverse cardiovascular events (composite of MI, ischemic stroke, or cardiovascular death). Included were 17 464 patients (63% men; mean age, 72.6 years) with a median hs CRP level of 2.2 (interquartile range, 1.0-6.0) mg/L and a median of 2.2 (interquartile range, 0.8-4.9) years since their MI . Most (66%) had hs CRP ≥2 mg/L, and 40% had hs CRP >3 mg/L. Lower hemoglobin, lower estimated glomerular filtration rate, and comorbidities (eg, heart failure, peripheral vascular disease, stroke, atrial fibrillation, diabetes mellitus, and rheumatoid diseases) were associated with higher odds of hs CRP ≥2 mg/L. Conversely, previous percutaneous coronary intervention, ongoing renin-angiotensin blockade, and statins were associated with lower hs CRP ≥2 mg/L odds. Patients with hs CRP ≥2 mg/L were at higher risk of major adverse cardiovascular events (n=3900; adjusted hazard ratio, 1.28; 95% CI, 1.18-1.38) and death (n=4138; adjusted hazard ratio, 1.42; 95% CI, 1.31-1.53). Results were robust across subgroups of patients and after exclusion of events occurring during the first 6 to 12 months. On a continuous scale, the association between hs CRP and outcomes was linear until hs CRP >5 mg/L, plateauing thereafter. Conclusions Most patients with MI exhibit elevated hs CRP levels. Besides identifying populations at high-inflammatory risk, this study extends the prognostic validity of this biomarker from trial evidence to real-world healthcare settings.
在临床试验的受控环境之外,关于心肌梗死(MI)患者“真实世界”中升高的 hs CRP(高敏 C 反应蛋白)的负担、预测因素和结局的信息很少。
我们纳入了在瑞典斯德哥尔摩的常规医疗保健中,在 MI 后 30 天以上进行 hs CRP 检测的所有 MI 幸存者(2006-2011 年)。排除了住院/急诊就诊期间进行的 hs CRP 检测、随后使用抗生素或提示急性疾病的 hs CRP 检测,以及正在接受治疗/近期患有癌症、慢性感染或免疫抑制的患者。炎症在 3 个月的基线窗口内定义,并与随后的死亡和主要不良心血管事件(MI、缺血性卒中和心血管死亡的复合终点)相关。共纳入 17464 例患者(63%为男性;平均年龄 72.6 岁),hs CRP 中位数为 2.2(四分位距,1.0-6.0)mg/L,MI 后中位数为 2.2(四分位距,0.8-4.9)年。大多数(66%)患者的 hs CRP≥2mg/L,40%患者的 hs CRP>3mg/L。较低的血红蛋白、较低的估算肾小球滤过率和合并症(如心力衰竭、外周血管疾病、卒中等)与 hs CRP≥2mg/L 的可能性更高相关。相反,先前的经皮冠状动脉介入治疗、持续的肾素-血管紧张素阻断和他汀类药物治疗与 hs CRP≥2mg/L 的可能性降低相关。hs CRP≥2mg/L 的患者发生主要不良心血管事件(n=3900;调整后的危险比,1.28;95%CI,1.18-1.38)和死亡(n=4138;调整后的危险比,1.42;95%CI,1.31-1.53)的风险更高。结果在患者亚组和排除前 6 至 12 个月内发生的事件后仍然稳健。在连续量表上,hs CRP 与结局之间的关联呈线性,直到 hs CRP>5mg/L,此后趋于平稳。
大多数 MI 患者表现出升高的 hs CRP 水平。除了确定高炎症风险人群外,本研究还将该生物标志物的预后有效性从试验证据扩展到真实世界的医疗保健环境。