Inserm 3iHP, CHU Clermont-Ferrand, Service d'Hépato-Gastro Entérologie, Université Clermont Auvergne, Clermont-Ferrand F-63000, France.
Biochemistry laboratory, University Hospital G. Montpied, Clermont-Ferrand F-63000, France.
World J Gastroenterol. 2019 May 21;25(19):2354-2364. doi: 10.3748/wjg.v25.i19.2354.
The individual performances and the complementarity of Crohn's disease (CD) activity index (CDAI), C-reactive protein (CRP) and faecal calprotectin (Fcal) to monitor patients with CD remain poorly investigated in the era of "tight control" and "treat to target" strategies.
To assess CDAI, CRP and Fcal variation, alone or combined, after 12 wk (W12) of anti-tumor necrosis factor (TNF) therapy to predict corticosteroids-free remission (CFREM = CDAI < 150, CRP < 2.9 mg/L and Fcal < 250 μg/g with no therapeutic intensification and no surgery) at W52.
CD adult patients needing anti-TNF therapy with CDAI > 150 and either CRP > 2.9 mg/L or Fcal > 250 μg/g were prospectively enrolled.
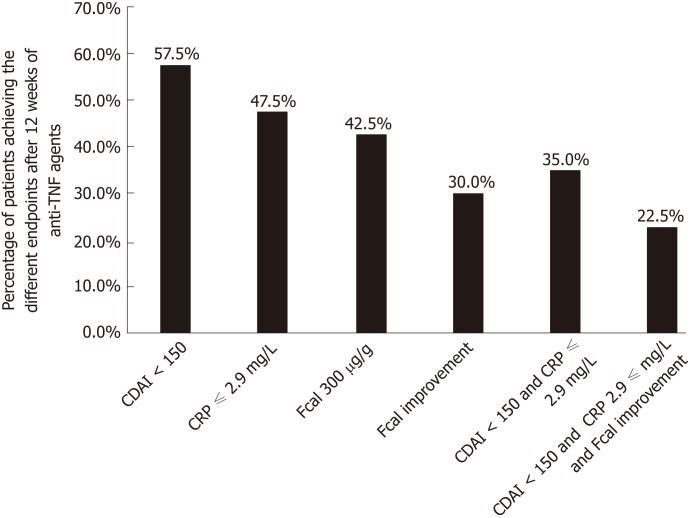
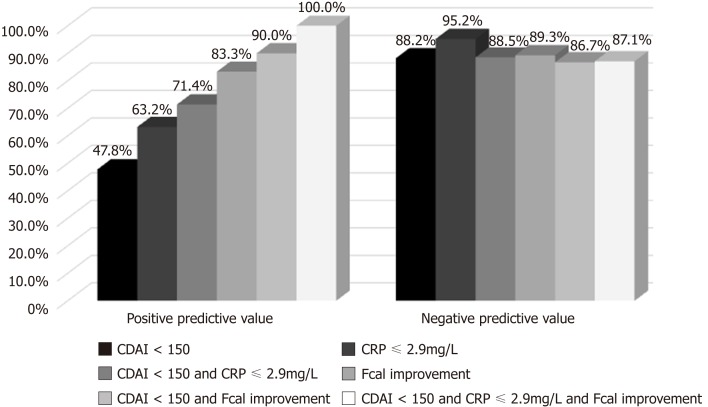
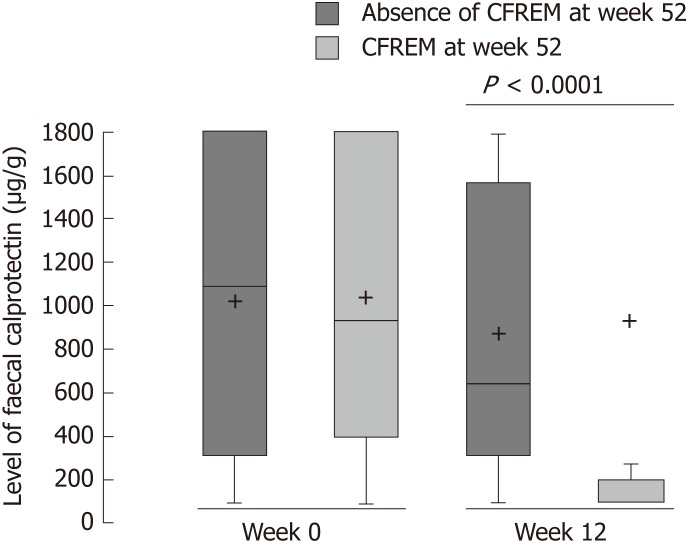
Among the 40 included patients, 13 patients (32.5%) achieved CFREM at W52. In univariable analysis, CDAI < 150 at W12 ( = 0.012), CRP level < 2.9 mg/L at W12 ( = 0.001) and Fcal improvement at W12 (Fcal < 300 μg/g; or, for patients with initial Fcal < 300 μg/g, at least 50% decrease of Fcal or normalization of Fcal (< 100 μg/g) ( = 0.001) were predictive of CFREM at W52. Combined endpoint (CDAI < 150 and CRP ≤ 2.9 mg/L and FCal improvement) at W12 was the best predictor of CFREM at W52 with positive predictive value = 100.0% (100.0-100.0) and negative predictive value = 87.1% (75.3-98.9). In multivariable analysis, Fcal improvement at W12 [odd ratio (OR) = 45.1 (2.96-687.9); = 0.03] was a better predictor of CFREM at W52 than CDAI < 150 [OR = 9.3 (0.36-237.1); = 0.145] and CRP < 2.9 mg/L (0.77-278.0; = 0.073).
The combined monitoring of CDAI, CRP and Fcal after anti-TNF induction therapy is able to predict favorable outcome within one year in patients with CD.
在“严格控制”和“治疗目标”策略的时代,个体表现和克罗恩病(CD)活动指数(CDAI)、C 反应蛋白(CRP)和粪便钙卫蛋白(Fcal)的互补性仍未得到充分研究,以监测 CD 患者。
评估抗肿瘤坏死因子(TNF)治疗 12 周(W12)后 CDAI、CRP 和 Fcal 的变化,单独或联合预测 52 周时无皮质类固醇缓解(CFREM = CDAI<150、CRP<2.9mg/L 和 Fcal<250μg/g,无治疗强化和无手术)。
前瞻性纳入需要抗 TNF 治疗且 CDAI>150 且 CRP>2.9mg/L 或 Fcal>250μg/g 的成年 CD 患者。
在 40 例纳入患者中,13 例(32.5%)在 52 周时达到 CFREM。单变量分析显示,W12 时 CDAI<150( = 0.012)、W12 时 CRP 水平<2.9mg/L( = 0.001)和 Fcal 改善(Fcal<300μg/g;或对于初始 Fcal<300μg/g 的患者,Fcal 降低至少 50%或 Fcal 正常化(<100μg/g)( = 0.001)预测 52 周时 CFREM。W12 时联合终点(CDAI<150、CRP≤2.9mg/L 和 FCal 改善)是预测 52 周 CFREM 的最佳指标,阳性预测值为 100.0%(100.0-100.0),阴性预测值为 87.1%(75.3-98.9)。多变量分析显示,W12 时 Fcal 改善[比值比(OR)=45.1(2.96-687.9); = 0.03]是预测 52 周 CFREM 的更好指标,优于 CDAI<150[OR=9.3(0.36-237.1); = 0.145]和 CRP<2.9mg/L(0.77-278.0; = 0.073)。
抗 TNF 诱导治疗后 CDAI、CRP 和 Fcal 的联合监测能够预测 CD 患者一年内的良好结果。