Centre for Inherited Cardiovascular Diseases, Great Ormond Street Hospital, Great Ormond Street, London, UK.
Institute of Cardiovascular Sciences University College London, London, UK.
Europace. 2019 Oct 1;21(10):1559-1565. doi: 10.1093/europace/euz118.
Sudden cardiac death (SCD) is the most common cause of death in children with hypertrophic cardiomyopathy (HCM). The European Society of Cardiology (ESC) recommends consideration of an implantable cardioverter-defibrillator (ICD) if two or more clinical risk factors (RFs) are present, but this approach to risk stratification has not been formally validated.
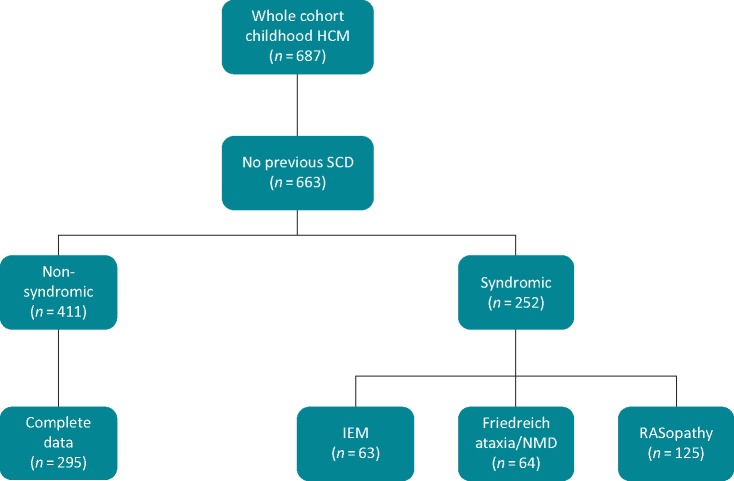
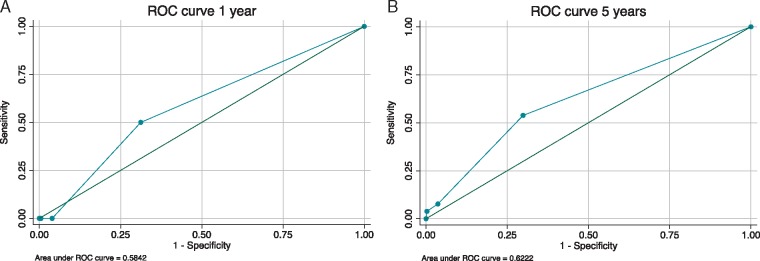
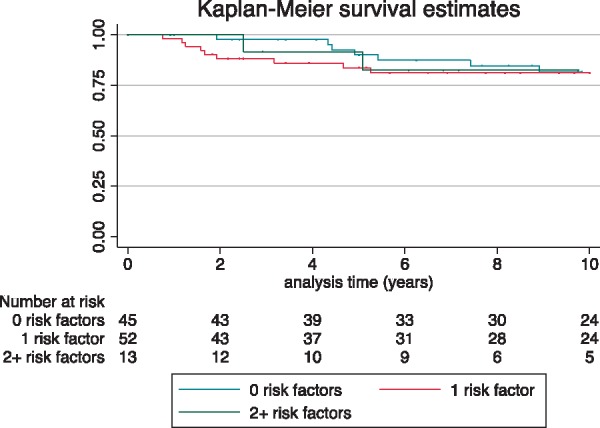
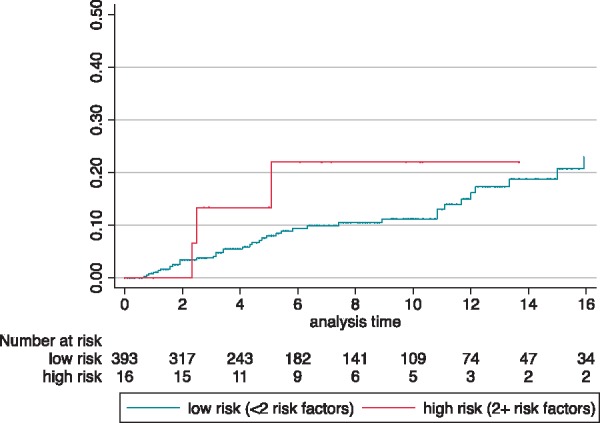
Four hundred and eleven paediatric HCM patients were assessed for four clinical RFs in accordance with current ESC recommendations: severe left ventricular hypertrophy, unexplained syncope, non-sustained ventricular tachycardia, and family history of SCD. The primary endpoint was a composite outcome of SCD or an equivalent event (aborted cardiac arrest, appropriate ICD therapy, or sustained ventricular tachycardia), defined as a major arrhythmic cardiac event (MACE). Over a follow-up period of 2890 patient years (median 5.5 years), MACE occurred in 21 patients (7.5%) with 0 RFs, 19 (16.8%) with 1 RFs, and 3 (18.8%) with 2 or more RFs. Corresponding incidence rates were 1.13 [95% confidence interval (CI) 0.7-1.73], 2.07 (95% CI 1.25-3.23), and 2.52 (95% CI 0.53-7.35) per 100 patient years at risk. Patients with two or more RFs did not have a higher incidence of MACE (log-rank test P = 0.34), with a positive and negative predictive value of 19% and 90%, respectively. The C-statistic was 0.62 (95% CI 0.52-0.72) at 5 years.
The incidence of MACE is higher for patients with increasing numbers of clinical RFs. However, the current ESC guidelines have a low ability to discriminate between high- and low-risk individuals.
心源性猝死(SCD)是肥厚型心肌病(HCM)患儿死亡的最常见原因。欧洲心脏病学会(ESC)建议,如果存在两个或更多临床风险因素(RFs),则考虑植入式心脏复律除颤器(ICD),但这种风险分层方法尚未得到正式验证。
根据当前 ESC 建议,对 411 例儿科 HCM 患者进行了四个临床 RFs 的评估:严重左心室肥厚、不明原因晕厥、非持续性室性心动过速和 SCD 家族史。主要终点是 SCD 或同等事件(心搏骤停、适当的 ICD 治疗或持续性室性心动过速)的复合结局,定义为主要心律失常性心脏事件(MACE)。在 2890 患者年的随访期间(中位数为 5.5 年),0 RFs 的 21 例患者(7.5%)、1 RFs 的 19 例患者(16.8%)和 2 个或更多 RFs 的 3 例患者(18.8%)发生 MACE。相应的发生率为每 100 患者年风险 1.13 [95%置信区间(CI)0.7-1.73]、2.07(95% CI 1.25-3.23)和 2.52(95% CI 0.53-7.35)。风险较高的患者(log-rank 检验 P=0.34)没有更高的 MACE 发生率,阳性和阴性预测值分别为 19%和 90%。5 年时的 C 统计量为 0.62(95% CI 0.52-0.72)。
随着临床 RFs 数量的增加,MACE 的发生率更高。然而,当前的 ESC 指南在区分高危和低危个体方面能力较低。