Center for Global Surgery Evaluation and Department of Otolaryngology, Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA, USA; Program in Global Surgery and Social Change, Harvard Medical School, Boston, MA, USA.
Program in Global Surgery and Social Change, Harvard Medical School, Boston, MA, USA; Department of Surgery, University of California Davis Medical Center, Davis, CA, USA.
Lancet Glob Health. 2019 Jul;7(7):e932-e939. doi: 10.1016/S2214-109X(19)30170-6.
Health-care regionalisation, in which selected services are concentrated in higher-level facilities, has successfully improved the quality of complex medical care. However, the effectiveness of this strategy in routine maternal care is unknown. Malawi has established a national goal of halving its neonatal mortality by 2030. In this study, we aimed to assess the effect of obstetric service regionalisation in pregnant women and their newborn babies in Malawi.
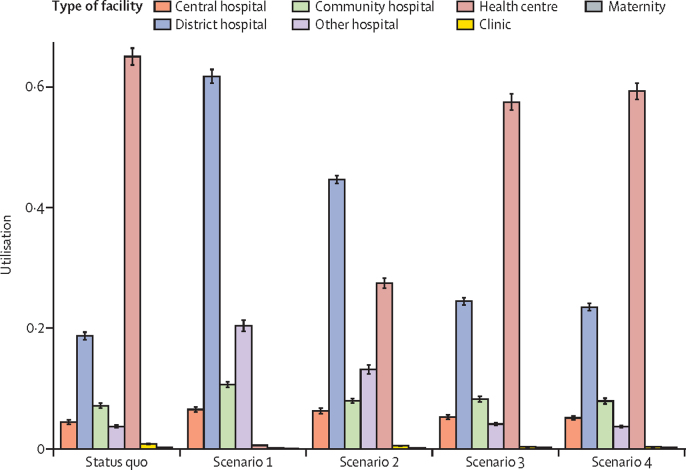
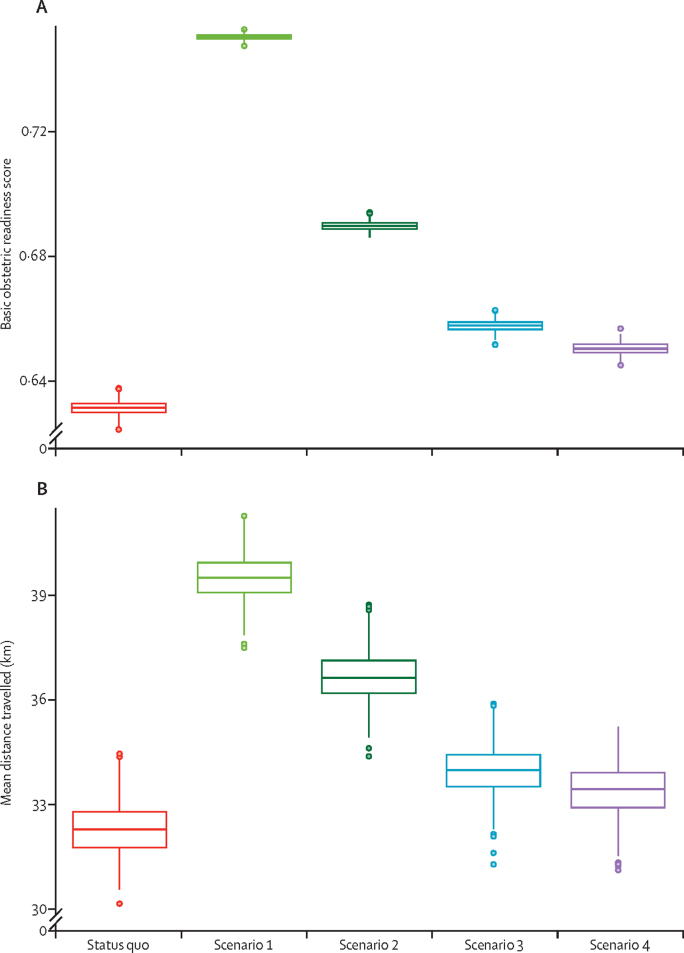
In this analysis, we assessed regionalisation through the use of an agent-based simulation model. We used a previously estimated utilisation function, incorporating both patient-specific and health-facility-specific characteristics, to inform patient choice. The model was validated against known utilisation patterns in Malawi. Four regionalisation scenarios were compared with the status quo: scenario 1 restricted deliveries to facilities currently capable of providing caesarean sections; scenario 2 had the same restrictions as scenario 1, but with selected facilities upgraded to provide caesarean sections; scenario 3 restricted delivery to facilities that provided five or more basic emergency obstetric and neonatal care services in the preceding 3 months; and scenario 4 had the same restrictions as scenario 3, but with selected facilities upgraded to provide at least five basic emergency obstetric and neonatal care services. We assessed neonatal mortality, utilisation, travel distance, median out-of-pocket expenditure, and proportion of women facing catastrophic expenditure. The effects of upgrading the obstetric readiness of all facilities, of removing all user fees, and of upgrading without restriction were considered in scenario analyses. Heterogeneity and parameter uncertainty were incorporated to create 95% posterior credible intervals (PCIs).
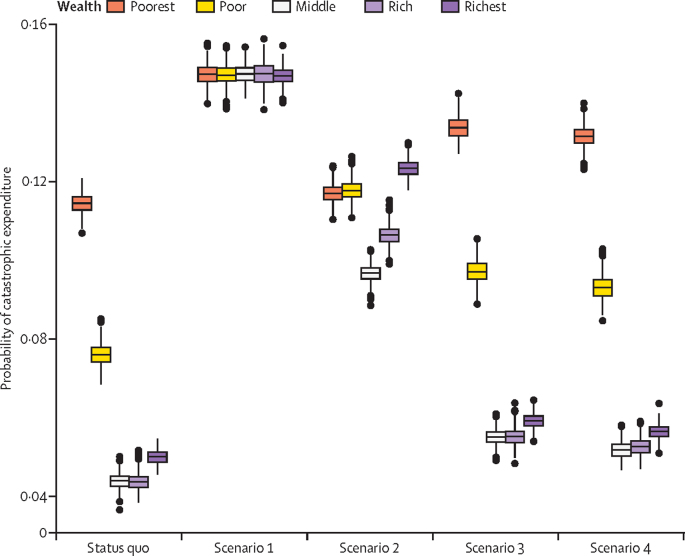
Scenarios restricting women to give birth in facilities with caesarean section capabilities reduced neonatal mortality by 11·4 deaths per 1000 livebirths (scenario 1; 95% PCI 9·8-13·1) and 11·6 deaths per 1000 livebirths (scenario 2; 10·2-13·1), whereas scenarios restricting women to facilities that provided five or more basic emergency obstetric and neonatal care services did not affect neonatal mortality. Similarly, the caesarean section rate in Malawi, which is 4·6% under the status quo, was predicted to rise significantly in scenario 1 (14·7%, 95% PCI 14·5-14·9; p<0·0001) and scenario 2 (10·4%, 10·2-10·6; p<0·0001), but not in scenarios 3 and 4. Women were required to travel longer distances in scenario 1 (increase of 7·2 km, 95% PCI 4·5-9·9) and in scenario 2 (4·4 km, 1·5-7·2) than in the status quo (p<0·0001). Out-of-pocket costs tripled (p<0·0001; status quo vs scenario 1 and scenario 2), and the risk of catastrophic expenditure significantly increased from a baseline of 6·4% (95% PCI 6·1-6·6) to 14·7% (14·5-14·9) in scenario 1 and 11·3% (11·0-11·5) in scenario 2. This increase was especially pronounced among the poor (p<0·0001; status quo vs scenario 1 and scenario 2).
Policies restricting women to give birth in facilities with caesarean section capabilities is likely to result in significant decreases in neonatal mortality and might allow Malawi to meet its goal of halving its neonatal mortality by 2030. However, this improvement comes at the cost of increased distances to care and worsening financial risks among women.
Bill & Melinda Gates Foundation, Damon Runyon Cancer Research Foundation.
在选定的服务集中在更高水平的设施中进行医疗区域化,已成功提高了复杂医疗护理的质量。然而,这种策略在常规产妇护理中的有效性尚不清楚。马拉维已制定了到 2030 年将新生儿死亡率减半的国家目标。在这项研究中,我们旨在评估在马拉维孕妇及其新生儿中实施产科服务区域化的效果。
在这项分析中,我们通过使用基于代理的模拟模型来评估区域化。我们使用了先前估计的利用函数,其中包含了患者特定和卫生设施特定的特征,以告知患者选择。该模型经过验证,与马拉维已知的利用模式相符。将四种区域化方案与现状进行比较:方案 1 将分娩限制在目前能够提供剖宫产的设施中;方案 2 具有与方案 1 相同的限制,但选择设施升级以提供剖宫产;方案 3 将分娩限制在过去 3 个月提供 5 种或更多基本紧急产科和新生儿护理服务的设施中;方案 4 具有与方案 3 相同的限制,但选择设施升级以提供至少 5 种基本紧急产科和新生儿护理服务。我们评估了新生儿死亡率、利用率、旅行距离、中位数自费支出以及面临灾难性支出的妇女比例。在方案分析中考虑了升级所有产科准备能力、取消所有用户费用以及升级不受限制的效果。纳入了异质性和参数不确定性,以创建 95%后验可信区间(PCIs)。
将妇女限制在具有剖宫产能力的设施中分娩的方案将新生儿死亡率降低了 11.4 例/每 1000 例活产(方案 1;95%PCIs 9.8-13.1)和 11.6 例/每 1000 例活产(方案 2;10.2-13.1),而将妇女限制在提供 5 种或更多基本紧急产科和新生儿护理服务的设施中并不影响新生儿死亡率。同样,在现状下,剖宫产率为 4.6%,在方案 1(14.7%,95%PCIs 14.5-14.9;p<0.0001)和方案 2(10.4%,10.2-10.6;p<0.0001)中,预计会显著上升,但在方案 3 和 4 中不会上升。与现状相比,方案 1(增加 7.2 公里,95%PCIs 4.5-9.9)和方案 2(4.4 公里,1.5-7.2)中妇女需要旅行更长的距离(p<0.0001)。自费支出增加了两倍(p<0.0001;现状与方案 1 和方案 2 相比),灾难性支出的风险从基线的 6.4%(95%PCIs 6.1-6.6)显著增加到方案 1 中的 14.7%(14.5-14.9)和方案 2 中的 11.3%(11.0-11.5)。这种增加在贫困人口中尤为明显(p<0.0001;现状与方案 1 和方案 2 相比)。
将妇女限制在具有剖宫产能力的设施中分娩的政策可能会显著降低新生儿死亡率,并使马拉维有可能实现到 2030 年将新生儿死亡率减半的目标。然而,这种改善是以增加护理距离和增加妇女的财务风险为代价的。
比尔及梅琳达·盖茨基金会、达蒙·鲁尼恩癌症研究基金会。