Kaiser Permanente Washington, Seattle.
Kaiser Permanente Washington Health Research Institute, Seattle.
JAMA Netw Open. 2019 Jul 3;2(7):e196570. doi: 10.1001/jamanetworkopen.2019.6570.
Colorectal cancer screening rates are suboptimal, particularly among sociodemographically disadvantaged groups.
To examine whether guaranteed money or probabilistic lottery financial incentives conditional on completion of colorectal cancer screening increase screening uptake, particularly among groups with lower screening rates.
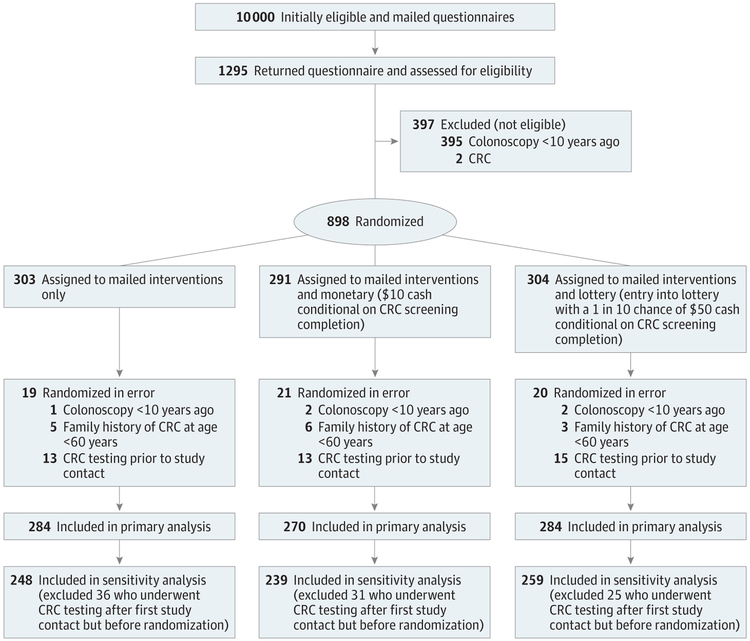
DESIGN, SETTING, AND PARTICIPANTS: This parallel, 3-arm randomized clinical trial was conducted from March 13, 2017, through April 12, 2018, at 21 medical centers in an integrated health care system in western Washington. A total of 838 age-eligible patients overdue for colorectal cancer screening who completed a questionnaire that confirmed eligibility and included sociodemographic and psychosocial questions were enrolled.
Interventions were (1) mail only (n = 284; up to 3 mailings that included information on the importance of colorectal cancer screening and screening test choices, a fecal immunochemical test [FIT], and a reminder letter if necessary), (2) mail and monetary (n = 270; mailings plus guaranteed $10 on screening completion), or (3) mail and lottery (n = 284; mailings plus a 1 in 10 chance of receiving $50 on screening completion).
The primary outcome was completion of any colorectal cancer screening within 6 months of randomization. Secondary outcomes were FIT or colonoscopy completion within 6 months of randomization. Intervention effects were compared across sociodemographic subgroups and self-reported psychosocial measures.
A total of 838 participants (mean [SD] age, 59.7 [7.2] years; 546 [65.2%] female; 433 [52.2%] white race and 101 [12.1%] Hispanic ethnicity) were included in the study. Completion of any colorectal screening was not significantly higher for the mail and monetary group (207 of 270 [76.7%]) or the mail and lottery group (212 of 284 [74.6%]) than for the mail only group (203 of 284 [71.5%]) (P = .11). For FIT completion, interventions had a statistically significant effect (P = .04), with a net increase of 7.7% (95% CI, 0.3%-15.1%) in the mail and monetary group and 7.1% (95% CI, -0.2% to 14.3%) in the mail and lottery group compared with the mail only group. For patients with Medicaid insurance, the net increase compared with mail only in FIT completion for the mail and monetary or the mail and lottery group was 37.7% (95% CI, 11.0%-64.3%) (34.2% for the mail and monetary group and 40.4% for the mail and lottery group) compared with a net increase of only 5.6% (95% CI, -0.9% to 12.2%) among those not Medicaid insured (test for interaction P = .03).
Financial incentives increased FIT uptake but not overall colorectal cancer screening. Financial incentives may decrease screening disparities among some sociodemographically disadvantaged groups.
ClinicalTrials.gov identifier: NCT00697047.
结直肠癌筛查率不理想,特别是在社会人口统计学上处于不利地位的群体中。
研究有保障的资金或基于完成结直肠癌筛查的概率彩票金融激励是否会增加筛查率,特别是在筛查率较低的人群中。
设计、设置和参与者:这是一项平行的、3 臂随机临床试验,于 2017 年 3 月 13 日至 2018 年 4 月 12 日在华盛顿西部一个综合医疗系统的 21 家医疗中心进行。共纳入了 838 名年龄符合条件但未进行结直肠癌筛查的患者,他们完成了一份问卷,确认了符合条件的条件,并包括了社会人口统计学和心理社会问题。
干预措施包括(1)仅邮寄(n = 284;最多 3 次邮寄,包括结直肠癌筛查的重要性和筛查试验选择的信息、粪便免疫化学试验[FIT],以及必要时的提醒信)、(2)邮寄和货币(n = 270;邮寄加上完成筛查的保证$10)或(3)邮寄和彩票(n = 284;邮寄加上完成筛查有 1/10 的机会获得$50)。
主要结果是在随机分组后 6 个月内完成任何结直肠癌筛查。次要结果是在随机分组后 6 个月内完成 FIT 或结肠镜检查。干预效果在社会人口统计学亚组和自我报告的心理社会测量方面进行了比较。
共有 838 名参与者(平均[SD]年龄,59.7[7.2]岁;546[65.2%]女性;433[52.2%]白人种族和 101[12.1%]西班牙裔)被纳入研究。与仅邮寄组(203/284[71.5%])相比,邮寄和货币组(270/270[76.7%])或邮寄和彩票组(284/284[74.6%])完成任何结直肠癌筛查的比例均无显著提高(P = .11)。对于 FIT 完成情况,干预措施具有统计学意义(P = .04),与仅邮寄组相比,邮寄和货币组的净增加了 7.7%(95%CI,0.3%-15.1%),邮寄和彩票组的净增加了 7.1%(95%CI,-0.2%至 14.3%)。对于有医疗补助保险的患者,与仅邮寄相比,在 FIT 完成方面,邮寄和货币组或邮寄和彩票组的净增加分别为 37.7%(95%CI,11.0%-64.3%)(邮寄和货币组为 34.2%,邮寄和彩票组为 40.4%),而不是医疗保险未覆盖的患者的净增加仅为 5.6%(95%CI,-0.9%至 12.2%)(检验交互作用 P = .03)。
经济激励措施增加了 FIT 的使用率,但并未增加整体结直肠癌筛查率。经济激励措施可能会减少一些社会人口统计学上处于不利地位的群体中的筛查差异。
ClinicalTrials.gov 标识符:NCT00697047。