Division of Surgical Oncology, Department of Surgery, University of Wisconsin, Madison, WI; Wisconsin Institute for Surgical Outcomes Research, Department of Surgery, University of Wisconsin, Madison, WI.
Wisconsin Institute for Surgical Outcomes Research, Department of Surgery, University of Wisconsin, Madison, WI.
Clin Breast Cancer. 2019 Dec;19(6):e741-e747. doi: 10.1016/j.clbc.2019.05.014. Epub 2019 Jun 6.
Tumor size has historically been used to stage breast cancer and guide treatment recommendations. The importance of tumor biology in long-term outcomes is increasingly being acknowledged. No large studies have examined the relative roles of tumor size and receptor status on response to neoadjuvant chemotherapy (NAC) in breast cancer.
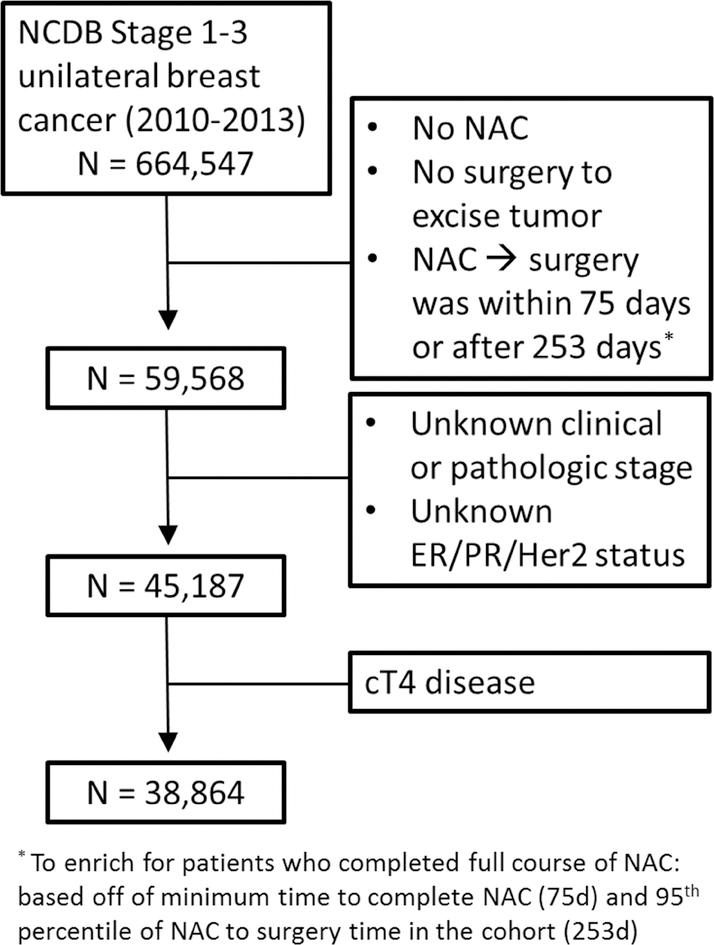
The National Cancer Database was queried for women who underwent NAC and surgery for unilateral clinical stage I to III (cT1-3) invasive breast cancer from 2010 to 2013. Multivariable logistic regression models were used to assess the relation between receptor status, tumor size, and pathologic complete response (pCR) while controlling for other biologic, sociodemographic, diagnosis, and treatment factors.
We included 38,864 women in this study, most presented with cT2 disease (55%). Patients predominantly had estrogen receptor (ER)/progesterone receptor (PR)-positive (ER/PR) HER2 (45%) or ER/PR HER2 (28%) disease. Nineteen percent (7432 patients) had a pCR. cT3 (odds ratio [OR], 0.64; 95% confidence interval [CI], 0.59-0.70) but not cT2 cancers (OR, 0.95; 95% CI, 0.89-1.02) were associated with lower pCR rates compared with cT1 disease. HER2 (ER/PR HER2: OR, 2.94; 95% CI, 2.72-3.18; ER/PR HER2: OR, 6.45; 95% CI, 5.92-7.02) and ER/PR HER2 cancers (OR, 3.94; 95% CI, 3.68-4.22) were more likely to experience pCR than those with ER/PR HER2 cancers. Receptor status was more strongly associated with pCR than tumor size.
Tumor size is independently associated with pCR after NAC after controlling for receptor status, although the effect of receptor status is stronger. These data reinforce the importance of receptor status as well as tumor size, each of which might act as surrogates for tumor biology, in setting expectations for outcomes in patients who undergo NAC.
肿瘤大小一直被用于分期乳腺癌并指导治疗建议。肿瘤生物学在长期预后中的重要性日益得到认可。目前尚无大型研究探讨肿瘤大小和受体状态对乳腺癌新辅助化疗(NAC)反应的相对作用。
本研究利用国家癌症数据库,检索了 2010 年至 2013 年期间接受单侧临床 I 期至 III 期(cT1-3)浸润性乳腺癌 NAC 及手术治疗的女性患者。采用多变量逻辑回归模型,在控制其他生物学、社会人口统计学、诊断和治疗因素的情况下,评估受体状态、肿瘤大小与病理完全缓解(pCR)之间的关系。
本研究共纳入 38864 例女性患者,多数为 cT2 疾病(55%)。患者主要为雌激素受体(ER)/孕激素受体(PR)阳性(ER/PR)HER2(45%)或 ER/PR HER2(28%)疾病。19%(7432 例)患者获得 pCR。与 cT1 疾病相比,cT3(比值比 [OR],0.64;95%置信区间 [CI],0.59-0.70)而不是 cT2 癌症(OR,0.95;95%CI,0.89-1.02)与较低的 pCR 率相关。与 ER/PR HER2 阳性癌症(OR,2.94;95%CI,2.72-3.18;ER/PR HER2 阳性癌症:OR,6.45;95%CI,5.92-7.02)相比,HER2(ER/PR HER2 阳性癌症:OR,2.94;95%CI,2.72-3.18;ER/PR HER2 阳性癌症:OR,6.45;95%CI,5.92-7.02)和 ER/PR HER2 阳性癌症(OR,3.94;95%CI,3.68-4.22)更有可能获得 pCR。受体状态与 pCR 的相关性强于肿瘤大小。
在控制受体状态后,肿瘤大小与 NAC 后 pCR 独立相关,尽管受体状态的影响更强。这些数据进一步证实了受体状态和肿瘤大小的重要性,两者均可能作为肿瘤生物学的替代指标,为接受 NAC 的患者设定预后期望。