Department of Physical Therapy, Faculty of Health Sciences, Ariel University, Ariel, Israel.
Department of Neurological Rehabilitation, Loewenstein Hospital, Raanana, Israel.
PLoS One. 2019 Jul 19;14(7):e0219738. doi: 10.1371/journal.pone.0219738. eCollection 2019.
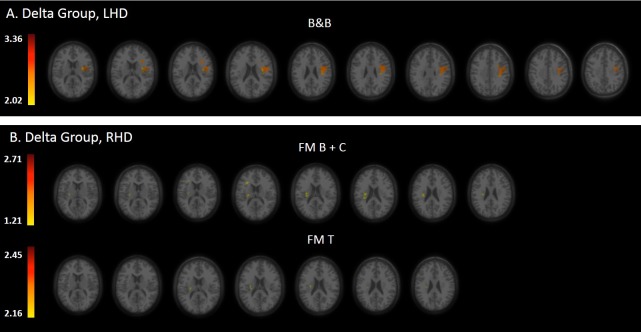
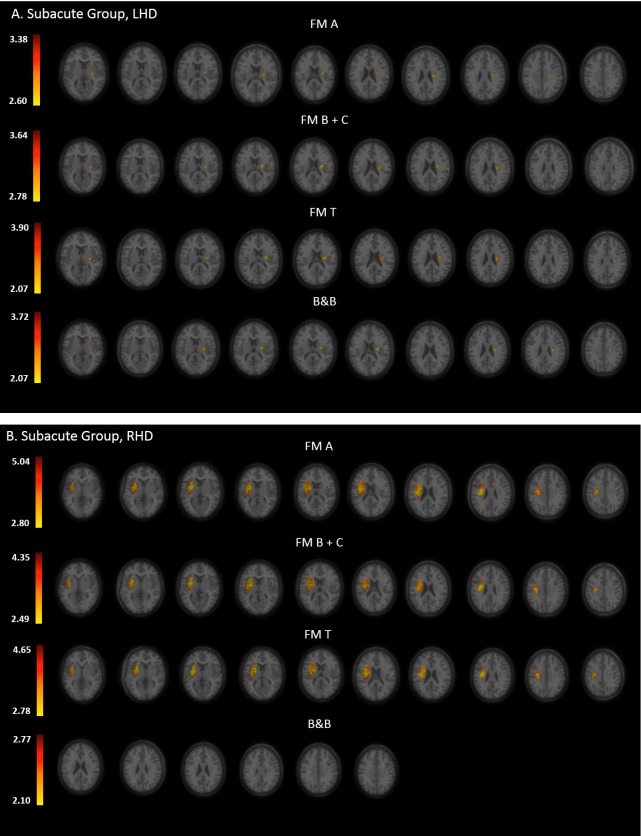
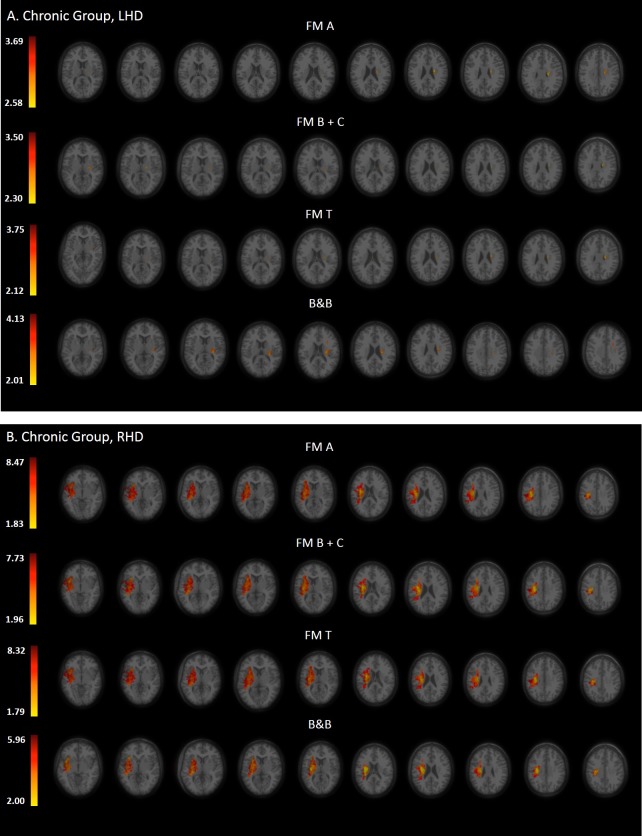
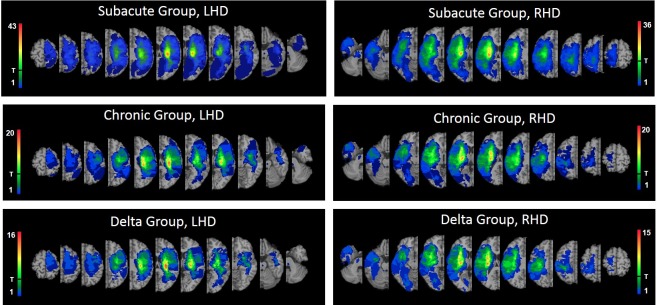
The effect of stroke topography on the recovery of hemiparetic upper limb (HUL) function is unclear due to limitations in previous studies-examination of lesion effects only in one point of time, or grouping together patients with left and right hemispheric damage (LHD, RHD), or disregard to different lesion impact on proximal and distal operations. Here we used voxel-based lesion symptom mapping (VLSM) to investigate the impact of stroke topography on HUL function taking into consideration the effects of (a) assessment time (subacute, chronic phases), (b) side of damaged hemisphere (left, right), (c) HUL part (proximal, distal). HUL function was examined in 3 groups of patients-Subacute (n = 130), Chronic (n = 66), and Delta (n = 49; patients examined both in the subacute and chronic phases)-using the proximal and distal sub-divisions of the Fugl-Meyer (FM) and the Box and Blocks (B&B) tests. HUL function following LHD tended to be affected in the subacute phase mainly by damage to white matter tracts, the putamen and the insula. In the chronic phase, a similar pattern was shown for B&B performance, whereas FM performance was affected by damage only to the white matter tracts. HUL function following RHD was affected in both phases, mainly by damage to the basal ganglia, white matter tracts and the insula, along with a restricted effect of damage to other cortical structures. In the chronic phase HUL function following RHD was affected also by damage to the thalamus. In the small Delta groups the following trends were found: In LHD patients, delayed motor recovery, captured by the B&B test, was affected by damage to the sensory-motor cortex, white matter association fibers and parts of the perisilvian cortex. In the RHD patients of the Delta group, delayed motor recovery was affected by damage to white matter projection fibers. Proximal and distal HUL functions examined in LHD patients (both in the subacute and chronic phases) tended to be affected by similar structures-mainly white matter projection tracts. In RHD patients, a distinction between proximal and distal HUL functions was found in the subacute but not in the chronic phase, with proximal and distal HUL functions affected by similar subcortical and cortical structures, except for an additional impact of damage to the superior temporal cortex and the retro-lenticular internal capsule only on proximal HUL function. The current study suggests the existence of important differences between the functional neuroanatomy underlying motor recovery following left and right hemisphere damage. A trend for different lesion effects was shown for residual proximal and distal HUL motor control. The study corroborates earlier findings showing an effect of the time after stroke onset (subacute, chronic) on the results of VLSM analyses. Further studies with larger sample size are required for the validation of these results.
由于先前研究的局限性,脑卒中部位对偏瘫上肢(HUL)功能恢复的影响尚不清楚 - 仅在一个时间点检查病变的影响,或对左侧和右侧半球损伤(LHD、RHD)进行分组,或不考虑不同病变对近端和远端操作的影响。在这里,我们使用基于体素的病变症状映射(VLSM)来研究脑卒中部位对 HUL 功能的影响,同时考虑到以下因素:(a)评估时间(亚急性期、慢性期),(b)损伤半球的侧别(左、右),(c)HUL 部位(近端、远端)。使用 Fugl-Meyer(FM)和 Box and Blocks(B&B)测试的近端和远端细分,对 3 组患者进行了 HUL 功能检查 - 亚急性期(n = 130)、慢性期(n = 66)和 Delta 期(n = 49;在亚急性期和慢性期均接受检查的患者)。LHD 后 HUL 功能在亚急性期主要受白质束、壳核和脑岛损伤的影响,在慢性期,B&B 表现也呈现出类似的模式,而 FM 表现仅受白质束损伤的影响。RHD 后 HUL 功能在两个阶段均受到影响,主要受基底节、白质束和脑岛损伤的影响,以及其他皮质结构损伤的限制作用。在慢性期,RHD 后 HUL 功能还受丘脑损伤的影响。在小 Delta 组中发现了以下趋势:在 LHD 患者中,B&B 测试检测到的运动恢复延迟,受感觉运动皮质、白质联络纤维和围脑岛皮质部分的损伤影响。在 RHD 患者的 Delta 组中,运动恢复延迟受白质投射纤维损伤的影响。LHD 患者(亚急性期和慢性期)检查的近端和远端 HUL 功能倾向于受类似结构的影响 - 主要是白质投射束。在 RHD 患者中,亚急性期存在近端和远端 HUL 功能之间的区别,但在慢性期则没有,近端和远端 HUL 功能受类似的皮质下和皮质结构影响,除了对颞上皮质和视束后内囊的损伤仅对近端 HUL 功能有额外影响外。目前的研究表明,左侧和右侧半球损伤后运动恢复的功能神经解剖存在重要差异。残留的近端和远端 HUL 运动控制的不同病变影响呈趋势。这项研究证实了先前的发现,即卒中后时间(亚急性期、慢性期)对 VLSM 分析结果有影响。需要进一步进行更大样本量的研究来验证这些结果。