Asokkumar Ravishankar, Yung Ka Chin, Loh Tracy, Kah Ling Lim, Gek San Tan, Ying Hao, Tan Damien, Khor Christopher, Lim Tony, Soetikno Roy
Department of Gastroenterology and Hepatology, Singapore General Hospital, Singapore.
Department of Anatomical Pathology, Singapore General Hospital, Singapore.
Endosc Int Open. 2019 Aug;7(8):E955-E963. doi: 10.1055/a-0903-2565. Epub 2019 Jul 24.
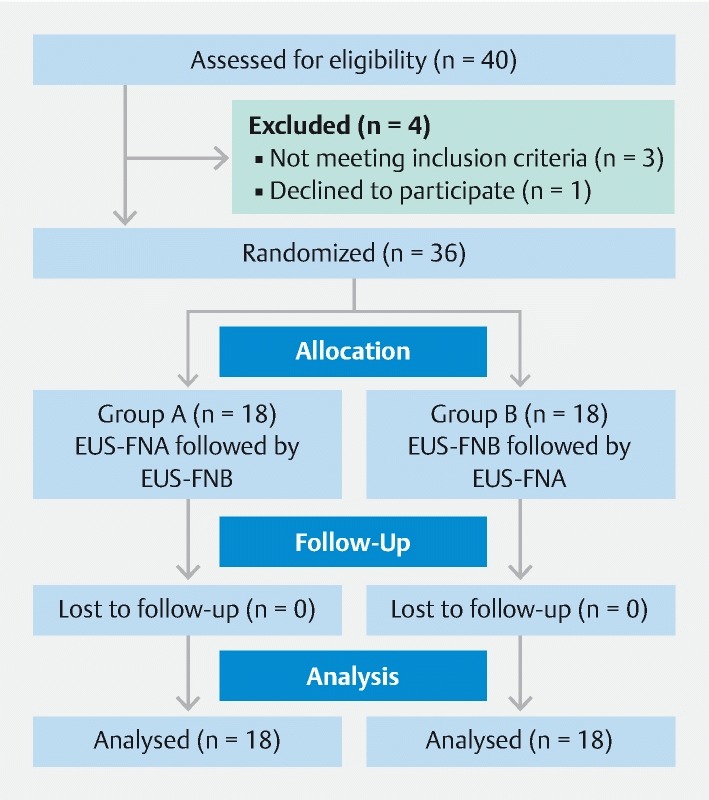
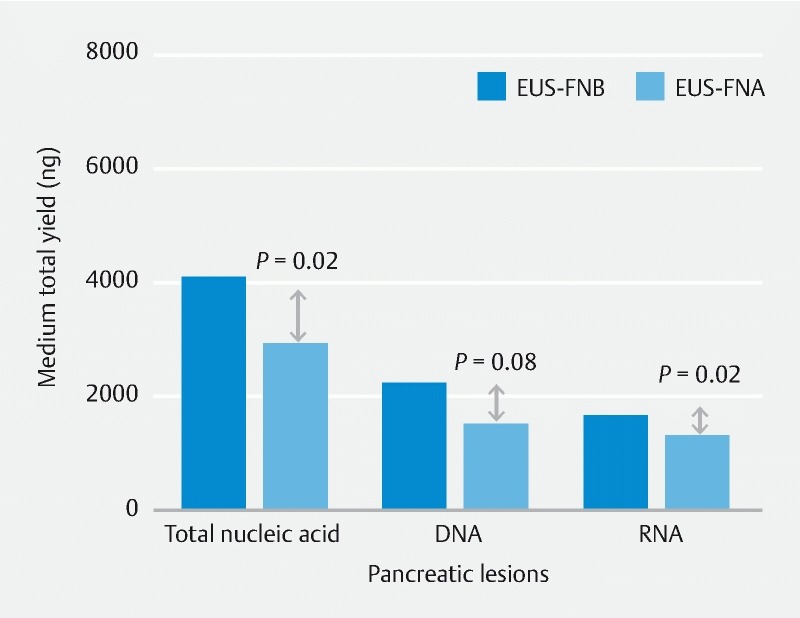
Recently, a new Franseen design endoscopic ultrasound-guided fine-needle biopsy (EUS-FNB) needle was developed with the goal of providing more tissue for histology. We compared the tissue adequacy rate and nucleic acid yield of 22G EUS-FNB vs. 22G endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA), in solid gastrointestinal and extra-intestinal lesions. We conducted a randomized crossover study and recruited 36 patients. We performed three passes for pancreatic lesions and two passes for other lesions, using each needle. We blinded the pathologist to needle assignment. We assessed the diagnostic tissue adequacy rate and compared the total tissue area, diagnostic tissue area, and desmoplastic stroma (DS) area in cases of carcinoma. We also examined the nucleic acid yield of the two needles in pancreatic lesions. The lesions included 20 pancreatic masses (55 %), six gastric subepithelial lesions (17 %), five lymph nodes (14 %) and five other abdominal masses (14 %). Mean ± SD lesion size was 3.8 ± 2.0 cm. The final diagnosis was malignant in 27 lesions (75 %) and benign in nine lesions (25 %). We found EUS-FNB procured significantly more median total tissue area (5.2 mm vs. 1.9 mm , < 0.001), diagnostic tissue area (2.2 mm vs. 0.9 mm , = 0.029), and DS area (2 mm vs. 0.1 mm , = 0.001) in lesions diagnosed as carcinoma (n = 23), as compared to EUS-FNA. In pancreatic lesions, EUS-FNB obtained significantly more nucleic acid than EUS-FNA (median; 4,085 ng vs. 2912 ng, = 0.02). There was no difference in the cellblock or rapid on-site cytological evaluation (ROSE) diagnostic yield between the needles. The 22G EUS-FNB provides more histological core tissue and adequate nucleic acid yield compared to 22G EUS-FNA. In this study, the diagnostic performance was similar between the needles.
最近,一种新的弗兰森设计的内镜超声引导下细针穿刺活检(EUS-FNB)针被研发出来,目的是获取更多用于组织学检查的组织。我们比较了22G EUS-FNB与22G内镜超声引导下细针抽吸术(EUS-FNA)在实体性胃肠道和肠外病变中的组织充足率和核酸产量。我们进行了一项随机交叉研究,招募了36名患者。对于胰腺病变,每种针均进行3次穿刺;对于其他病变,进行2次穿刺。我们对病理学家隐瞒针的分配情况。我们评估了诊断性组织充足率,并比较了癌病例中的总组织面积、诊断性组织面积和促纤维组织增生性间质(DS)面积。我们还检测了两种针在胰腺病变中的核酸产量。病变包括20个胰腺肿块(55%)、6个胃上皮下病变(17%)、5个淋巴结(14%)和5个其他腹部肿块(14%)。病变的平均大小±标准差为3.8±2.0cm。最终诊断为恶性的病变有27个(75%),良性的有9个(25%)。我们发现,与EUS-FNA相比,在诊断为癌的病变(n = 23)中,EUS-FNB获取的中位总组织面积(5.2mm²对1.9mm²,P < 0.001)、诊断性组织面积(2.2mm²对0.9mm²,P = 0.029)和DS面积(2mm²对0.1mm²,P = 0.001)显著更多。在胰腺病变中,EUS-FNB获得的核酸明显多于EUS-FNA(中位值;4085ng对2912ng,P = 0.02)。两种针在细胞块或快速现场细胞学评估(ROSE)诊断率方面没有差异。与22G EUS-FNA相比,22G EUS-FNB能提供更多的组织学核心组织和充足的核酸产量。在本研究中,两种针的诊断性能相似。