Viveiros Pedro, Riaz Ahsun, Lewandowski Robert J, Mahalingam Devalingam
Developmental Therapeutics, Robert H. Lurie Comprehensive Cancer Center, Northwestern University Feinberg School of Medicine, Chicago, IL 60611, USA.
Department of Radiology, Northwestern University Feinberg School of Medicine, Chicago, IL 60611, USA.
Cancers (Basel). 2019 Jul 31;11(8):1085. doi: 10.3390/cancers11081085.
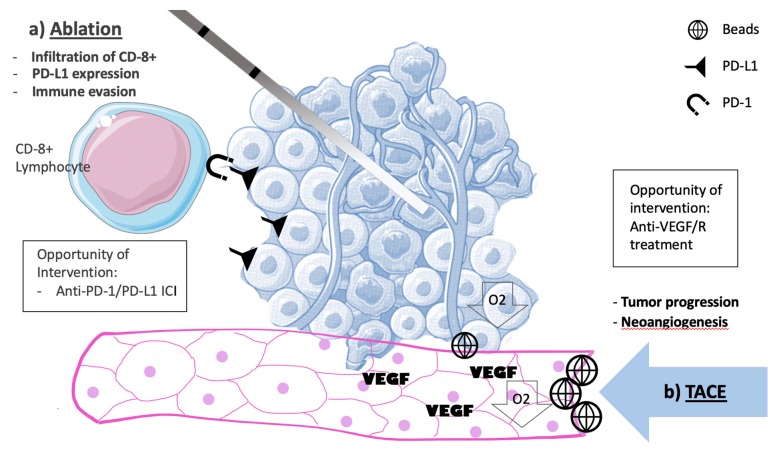
The increasing set of liver-directed therapies (LDT) have become an integral part of hepatocellular carcinoma (HCC) treatment. These range from percutaneous ablative techniques to arterial embolization, and varied radiotherapy strategies. They are now used for local disease control, symptom palliation, and bold curative strategies. The big challenge in the face of these innovative and sometimes overlapping technologies is to identify the best opportunity of use. In real practice, many patients may take benefit from LDT used as a bridge to curative treatment such as resection and liver transplantation. Varying trans-arterial embolization strategies are used, and comparison between established and developing technologies is scarce. Also, radioembolization utilizing yttrium-90 (Y-90) for locally advanced or intermediate-stage HCC needs further evidence of clinical efficacy. There is increasing interest on LDT-led changes in tumor biology that could have implications in systemic therapy efficacy. Foremost, additional to its apoptotic and necrotic properties, LDT could warrant changes in vascular endothelial growth factor (VEGF) expression and release. However, trans-arterial chemoembolization (TACE) used alongside tyrosine-kinase inhibitor (TKI) sorafenib has had its efficacy contested. Most recently, interest in associating Y-90 and TKI has emerged. Furthermore, LDT-led differences in tumor immune microenvironment and immune cell infiltration could be an opportunity to enhance immunotherapy efficacy for HCC patients. Early attempts to coordinate LDT and immunotherapy are being made. We here review LDT techniques exposing current evidence to understand its extant reach and future applications alongside systemic therapy development for HCC.
越来越多的肝脏定向治疗(LDT)已成为肝细胞癌(HCC)治疗不可或缺的一部分。这些治疗方法涵盖了从经皮消融技术到动脉栓塞以及各种放疗策略。它们现在用于局部疾病控制、症状缓解和大胆的根治性策略。面对这些创新且有时相互重叠的技术,最大的挑战是确定最佳的使用时机。在实际临床中,许多患者可能会受益于将LDT用作通向诸如切除和肝移植等根治性治疗的桥梁。目前采用了多种经动脉栓塞策略,但成熟技术与新兴技术之间的比较却很少。此外,利用钇-90(Y-9)进行放射性栓塞治疗局部晚期或中期HCC的临床疗效还需要更多证据。人们越来越关注LDT引发的肿瘤生物学变化,这可能会对全身治疗疗效产生影响。首先,除了其凋亡和坏死特性外,LDT可能会引起血管内皮生长因子(VEGF)表达和释放的变化。然而,经动脉化疗栓塞(TACE)与酪氨酸激酶抑制剂(TKI)索拉非尼联合使用的疗效存在争议。最近,将Y-90和TKI联合使用的研究引起了关注。此外,LDT导致的肿瘤免疫微环境和免疫细胞浸润差异可能是提高HCC患者免疫治疗疗效的一个契机。目前正在进行早期尝试以协调LDT和免疫治疗。我们在此回顾LDT技术,展示现有证据,以了解其目前的应用范围以及在HCC全身治疗发展背景下的未来应用。