Department of Public Health, Erasmus MC University Medical Centre, Rotterdam, the Netherlands.
Department of Neurology, Erasmus MC University Medical Centre, Rotterdam, the Netherlands.
Br J Surg. 2020 Mar;107(4):373-380. doi: 10.1002/bjs.11304. Epub 2019 Sep 10.
Patients with major trauma might benefit from treatment in a trauma centre, but early identification of major trauma (Injury Severity Score (ISS) over 15) remains difficult. The aim of this study was to undertake an external validation of existing prognostic models for injured patients to assess their ability to predict mortality and major trauma in the prehospital setting.
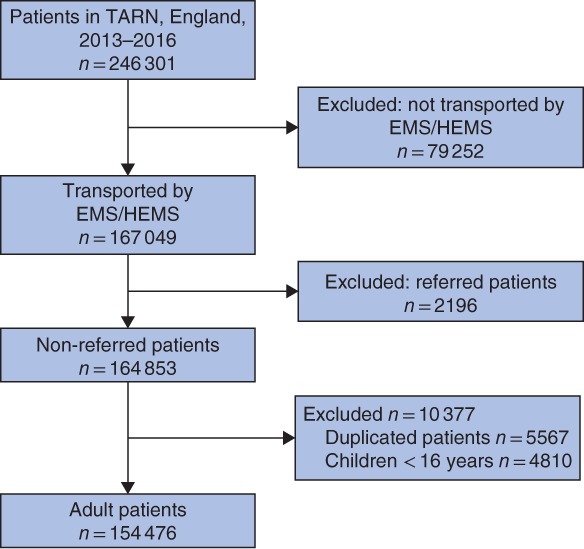
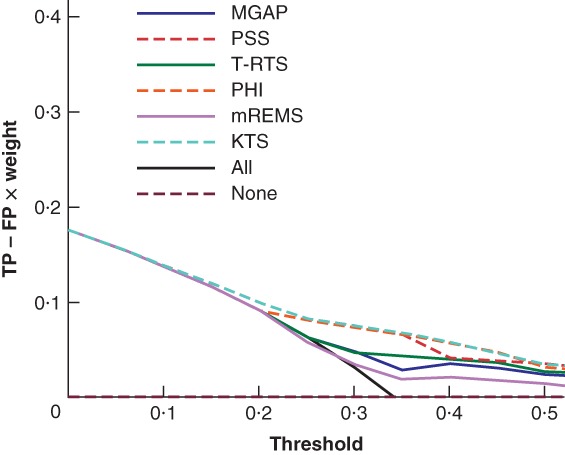
Prognostic models were identified through a systematic literature search up to October 2017. Injured patients transported by Emergency Medical Services to an English hospital from the Trauma Audit and Research Network between 2013 and 2016 were included. Outcome measures were major trauma (ISS over 15) and in-hospital mortality. The performance of the models was assessed in terms of discrimination (concordance index, C-statistic) and net benefit to assess the clinical usefulness.
A total of 154 476 patients were included to validate six previously proposed prediction models. Discriminative ability ranged from a C-statistic value of 0·602 (95 per cent c.i. 0·596 to 0·608) for the Mechanism, Glasgow Coma Scale, Age and Arterial Pressure model to 0·793 (0·789 to 0·797) for the modified Rapid Emergency Medicine Score (mREMS) in predicting in-hospital mortality (11 882 patients). Major trauma was identified in 52 818 patients, with discrimination from a C-statistic value of 0·589 (0·586 to 0·592) for mREMS to 0·735 (0·733 to 0·737) for the Kampala Trauma Score in predicting major trauma. None of the prediction models met acceptable undertriage and overtriage rates.
Currently available prehospital trauma models perform reasonably in predicting in-hospital mortality, but are inadequate in identifying patients with major trauma. Future research should focus on which patients would benefit from treatment in a major trauma centre.
严重创伤患者可能受益于创伤中心的治疗,但早期识别严重创伤(损伤严重程度评分(ISS)超过 15)仍然困难。本研究的目的是对现有的创伤患者预后模型进行外部验证,以评估其在院前环境下预测死亡率和严重创伤的能力。
通过系统文献检索,确定了截至 2017 年 10 月的预后模型。纳入 2013 年至 2016 年期间由紧急医疗服务机构转运至英国医院的创伤审核和研究网络中的受伤患者。结局指标为严重创伤(ISS 超过 15)和院内死亡率。通过判别能力(一致性指数,C 统计量)和净效益评估模型的性能,以评估临床实用性。
共纳入 154476 例患者对 6 个先前提出的预测模型进行验证。判别能力从机制、格拉斯哥昏迷评分、年龄和动脉压模型的 C 统计量值 0.602(95%可信区间 0.596-0.608)到改良快速急诊医学评分(mREMS)预测院内死亡率(11882 例患者)的 0.793(0.789-0.797)不等。52818 例患者被诊断为严重创伤,mREMS 的 C 统计量值为 0.589(0.586-0.592),坎帕拉创伤评分预测严重创伤的 C 统计量值为 0.735(0.733-0.737)。目前没有一种院前创伤模型能够满足可接受的分诊不足和过度分诊率。
目前可用的院前创伤模型在预测院内死亡率方面表现尚可,但在识别严重创伤患者方面不足。未来的研究应集中在哪些患者将受益于创伤中心的治疗。