Li Ryan, Hernandez-Villafuerte Karla, Towse Adrian, Vlad Ioana, Chalkidou Kalipso
NICE International, National Institute for Health and Care Excellence , London , UK.
Office of Health Economics , London , UK.
Health Syst Reform. 2016 Jan 2;2(1):71-83. doi: 10.1080/23288604.2015.1123338.
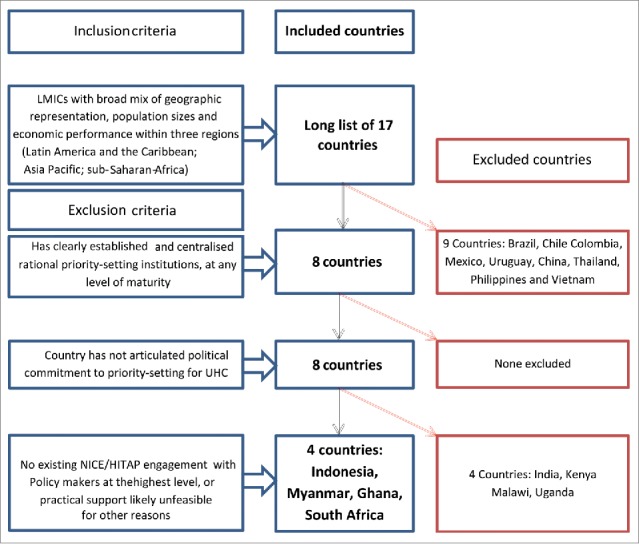
-As more low- and middle-income countries (LMICs) commit to universal health coverage (UHC), there is a growing need for rational priority setting using health technology assessment (HTA) and other policy tools. We describe an approach for rapidly mapping LMICs' capacity and needs for rational priority setting, aimed at identifying candidate countries where technical assistance would be most viable, and present our findings from applying this approach to three continents. Drawing on the multiple streams theory and a conceptual model of HTA in health systems, we developed qualitative and quantitative indicators for political commitment, current position along UHC journey, institutional and technical capacity, health system financing characteristics, and potential economies of scale in rational priority setting and associated data collection tools. We additionally defined criteria for shortlisting countries, emphasizing feasibility of technical assistance. We purposively sampled 17 countries and gathered data up to May 2014 from various sources and applied the shortlisting criteria to these countries. The four shortlisted countries (Indonesia, Myanmar, South Africa, Ghana) had varying capacities for rational priority setting and shared clear demand for rational priority setting as a means of achieving UHC. Indonesia was the strongest candidate for technical assistance, given the potential scale of impact on its large population and potential lessons for LMICs transitioning from aid. We conducted additional in-country scoping, and technical assistance to support HTA development in Indonesia is now underway. Our approach is of potential value to development funders and initiatives seeking to maximize the impact of their aid investments in support of UHC.
随着越来越多的低收入和中等收入国家(LMICs)致力于实现全民健康覆盖(UHC),利用卫生技术评估(HTA)和其他政策工具进行合理的优先事项设定的需求日益增长。我们描述了一种快速摸清LMICs进行合理优先事项设定的能力和需求的方法,旨在确定技术援助最可行的候选国家,并展示我们将该方法应用于三大洲的研究结果。借鉴多源流理论和卫生系统中HTA的概念模型,我们制定了关于政治承诺、在全民健康覆盖进程中的当前位置、机构和技术能力、卫生系统融资特征以及合理优先事项设定和相关数据收集工具中的潜在规模经济的定性和定量指标。我们还定义了入围国家的标准,强调技术援助的可行性。我们有目的地选取了17个国家,并从各种来源收集了截至2014年5月的数据,并将入围标准应用于这些国家。四个入围国家(印度尼西亚、缅甸、南非、加纳)在合理优先事项设定方面能力各异,并且都明确表示需要通过合理优先事项设定来实现全民健康覆盖。鉴于对其庞大人口的潜在影响规模以及对从援助转型的LMICs的潜在借鉴意义,印度尼西亚是技术援助的最强候选国家。我们进行了额外的国内范围界定,目前正在为支持印度尼西亚的HTA发展提供技术援助。我们的方法对于寻求最大限度地提高其援助投资对支持全民健康覆盖的影响的发展资助者和倡议具有潜在价值。