Vardiman Arnold B, Wallace David J, Booher Grant A, Crawford Neil R, Riggleman Jessica R, Greeley Samantha L, Ledonio Charles G
Department of Neurosurgery, University of Texas Health San Antonio, 7703 Floyd Curl Drive, MC 7843, San Antonio, TX, 78229-3900, USA.
A Division of Globus Medical, Inc, Musculoskeletal Education and Research Center (MERC), 2560 General Armistead Avenue, Audubon, PA, 19403, USA.
J Robot Surg. 2020 Aug;14(4):567-572. doi: 10.1007/s11701-019-01019-9. Epub 2019 Sep 21.
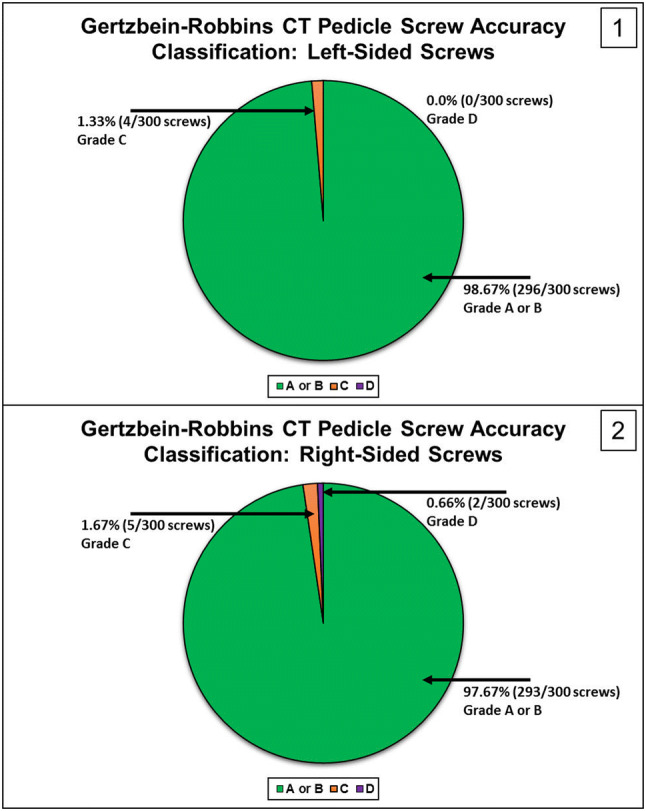
Robotic assistance with integrated navigation is an area of high interest for improving the accuracy of minimally invasive pedicle screw placement. This study analyzes the accuracy of pedicle screw placement between an attending spine surgeon and a resident by comparing the left and right sides of the first 101 consecutive cases using navigated robotic assistance in a private practice clinical setting. A retrospective, Institutional Review Board-exempt review of the first 106 navigated robot-assisted spine surgery cases was performed. One attending spine surgeon and one resident performed pedicle screw placement consistently on either the left or right side (researchers were blinded). A CT-based Gertzbein and Robbins system (GRS) was used to classify pedicle screw accuracy, with grade A or B considered accurate. There were 630 consecutive lumbosacral pedicle screws placed. Thirty screws (5 patients) were placed without the robot due to surgeon discretion. Of the 600 pedicle screws inserted by navigated robotic guidance (101 patients), only 1.5% (9/600) were repositioned intraoperatively. Based on the GRS CT-based grading of pedicle breach, 98.67% (296/300) of left-side screws were graded A or B, 1.3% (4/300) were graded C, and 0% (0/300) were graded D. For the right-side screws, 97.67% (293/300) were graded A or B, 1.67% (5/300) were graded C, and 0.66% (2/300) were graded D. This study demonstrated a high level of accuracy (based on GRS) with no significant differences between the left- and right-side pedicle screw placements (98.67% vs. 97.67%, respectively) in the clinical use of navigated, robot-assisted surgery.
集成导航的机器人辅助技术是提高微创椎弓根螺钉置入准确性的一个备受关注的领域。本研究通过在私人诊所临床环境中,对连续101例使用导航机器人辅助技术的病例的左右两侧进行比较,分析了脊柱主治医生和住院医生之间椎弓根螺钉置入的准确性。对前106例导航机器人辅助脊柱手术病例进行了回顾性、机构审查委员会豁免审查。一名脊柱主治医生和一名住院医生始终在左侧或右侧进行椎弓根螺钉置入(研究人员不知情)。使用基于CT的Gertzbein和Robbins系统(GRS)对椎弓根螺钉准确性进行分类,A级或B级视为准确。共连续置入630枚腰骶椎弓根螺钉。由于外科医生的决定,30枚螺钉(5例患者)在没有机器人辅助的情况下置入。在通过导航机器人引导置入的600枚椎弓根螺钉(101例患者)中,术中仅1.5%(9/600)需要重新定位。根据基于GRS CT的椎弓根穿孔分级,左侧螺钉98.67%(296/300)为A级或B级,1.3%(4/300)为C级,0%(0/300)为D级。右侧螺钉方面,97.67%(293/300)为A级或B级,1.67%(5/300)为C级,0.66%(2/300)为D级。本研究表明,在导航机器人辅助手术的临床应用中,准确性很高(基于GRS),左右侧椎弓根螺钉置入之间无显著差异(分别为98.67%和97.67%)。