Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
Center on Aging and Health, Johns Hopkins University and Medical Institutions, Baltimore, Maryland.
JAMA Netw Open. 2019 Oct 2;2(10):e1912352. doi: 10.1001/jamanetworkopen.2019.12352.
Fragmented daily physical activity may be a sign of physiological decline that provides more powerful insight into impending mortality than total daily activity.
To compare and contrast the association between total daily activity and activity fragmentation, which encompasses activity bouts and duration, and mortality risk.
DESIGN, SETTING, AND PARTICIPANTS: In this cohort study, accelerometer data from 2007 through 2015 and mortality data from 2007 through 2017 were collected from 548 adults aged 65 years and older participating in the Baltimore Longitudinal Study of Aging. The dates of analysis were November 2016 to June 2019, with data collected through December 31, 2017. Using Cox proportional hazards regression, the association between accelerometer-derived patterns of physical activity and mortality was estimated after adjusting for demographic characteristics, lifestyle factors, and comorbidities.
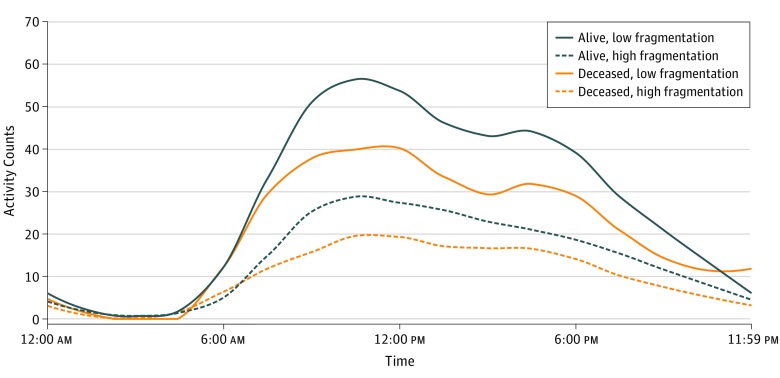
Minute-by-minute physical activity data were collected over a 24-hour, 7-day period (excluding times between 11:00 pm and 4:59 am) using an accelerometer. Each minute was labeled either active or sedentary, and 5 features of accelerometer data were extracted: total daily activity (defined as any activity performed throughout the day), activity fragmentation (defined as an active-to-sedentary transition probability), and 3 measures of activity bouts (<5, 5-10, and ≥10 active minutes).
All-cause mortality.
Among 548 well-functioning older adults (mean [SD] age, 75.8 [7.2] years; 262 [47.8%] women), 61 participants (11.1%) died. Total daily physical activity was not associated with mortality risk (hazard ratio [HR], 0.90 [95% CI, 0.75-1.08]; P = .28). However, more fragmented physical activity patterns were associated with greater mortality risk (HR, 1.49 [95% CI, 1.02-2.19]; P = .04) after adjusting for age, sex, race/ethnicity, body mass index, smoking history, employment, self-reported health, grip strength, usual gait speed, comorbidities, and device wear time. In addition, more frequently engaging in activity bouts lasting less than 5 minutes was associated with greater mortality risk (HR, 1.28 [95% CI, 1.01-1.61]; P = .04), whereas activity bouts of 5 to 10 minutes (HR, 0.99 [95% CI, 0.58-1.69]; P = .97) and 10 minutes or longer (HR, 0.81 [95% CI, 0.65-1.01]; P = .06) were not associated with mortality risk.
In this cohort study of well-functioning adults aged 65 years and older, fragmented daily physical activity, particularly activity bouts lasting less than 5 minutes, was associated with greater mortality risk. These findings suggest that activity fragmentation in older adults may precede declines in functional capability and overall physical activity that typically indicate impending mortality.
日常身体活动碎片化可能是生理衰退的一个迹象,它比日常总活动更能深入洞察即将发生的死亡。
比较和对比总日常活动与活动碎片化(包括活动片段和持续时间)与死亡率风险之间的关联。
设计、地点和参与者:在这项队列研究中,从 2007 年至 2015 年收集了加速度计数据,从 2007 年至 2017 年收集了死亡率数据,参与者为 548 名年龄在 65 岁及以上、参加巴尔的摩老龄化纵向研究的成年人。分析日期为 2016 年 11 月至 2019 年 6 月,数据收集截至 2017 年 12 月 31 日。使用 Cox 比例风险回归,在调整人口统计学特征、生活方式因素和合并症后,估计了加速度计得出的身体活动模式与死亡率之间的关联。
使用加速度计在 24 小时、7 天的时间内(不包括晚上 11:00 至凌晨 4:59 之间的时间)收集每分钟的身体活动数据。每分钟都被标记为活跃或静止,从加速度计数据中提取了 5 个特征:总日常活动(定义为全天进行的任何活动)、活动碎片化(定义为活跃到静止的转换概率)和 3 个活动片段的测量值(<5、5-10 和≥10 活跃分钟)。
全因死亡率。
在 548 名身体状况良好的老年人(平均[SD]年龄,75.8[7.2]岁;262[47.8%]名女性)中,有 61 名(11.1%)死亡。总日常体力活动与死亡率风险无关(风险比[HR],0.90[95%CI,0.75-1.08];P=0.28)。然而,调整年龄、性别、种族/民族、体重指数、吸烟史、就业、自我报告的健康状况、握力、通常的步行速度、合并症和设备佩戴时间后,更碎片化的身体活动模式与更高的死亡率风险相关(HR,1.49[95%CI,1.02-2.19];P=0.04)。此外,更频繁地进行持续时间小于 5 分钟的活动片段与更高的死亡率风险相关(HR,1.28[95%CI,1.01-1.61];P=0.04),而持续时间为 5 至 10 分钟的活动片段(HR,0.99[95%CI,0.58-1.69];P=0.97)和 10 分钟或更长时间的活动片段(HR,0.81[95%CI,0.65-1.01];P=0.06)与死亡率风险无关。
在这项对 65 岁及以上身体状况良好的成年人的队列研究中,日常身体活动碎片化,特别是持续时间小于 5 分钟的活动片段,与更高的死亡率风险相关。这些发现表明,老年人的活动碎片化可能先于功能能力和整体身体活动的下降,而这些下降通常预示着即将发生的死亡。