College of Health and Human Services, San Diego State University, San Diego, California.
Department of Medicine, Columbia University Irving Medical Center, New York, New York.
JAMA Netw Open. 2022 Jun 1;5(6):e2215385. doi: 10.1001/jamanetworkopen.2022.15385.
The amount and intensity of physical activity required to prevent stroke are yet to be fully determined because of previous reliance on self-reporting measures. Furthermore, the association between objectively measured time spent being sedentary as an independent risk factor for stroke is unknown.
To investigate the associations of accelerometer-measured sedentary time and physical activity of varying intensity and duration with the risk of incident stroke.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study involved participants who were enrolled in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study from February 5, 2003, to October 30, 2007. Accelerometer data were collected from 7607 Black and White adults 45 years or older in the contiguous US between May 12, 2009, and January 5, 2013. Data on other races and ethnicities were not collected for scientific and clinical reasons. By design, Black adults and residents of the southeastern US stroke belt and stroke buckle were oversampled. Data were analyzed from May 5, 2020, to November 11, 2021.
Sedentary time, light-intensity physical activity (LIPA), and moderate- to vigorous-intensity physical activity (MVPA) were measured using a hip-mounted accelerometer worn for 7 consecutive days and stratified by tertile for the analyses.
Incident stroke.
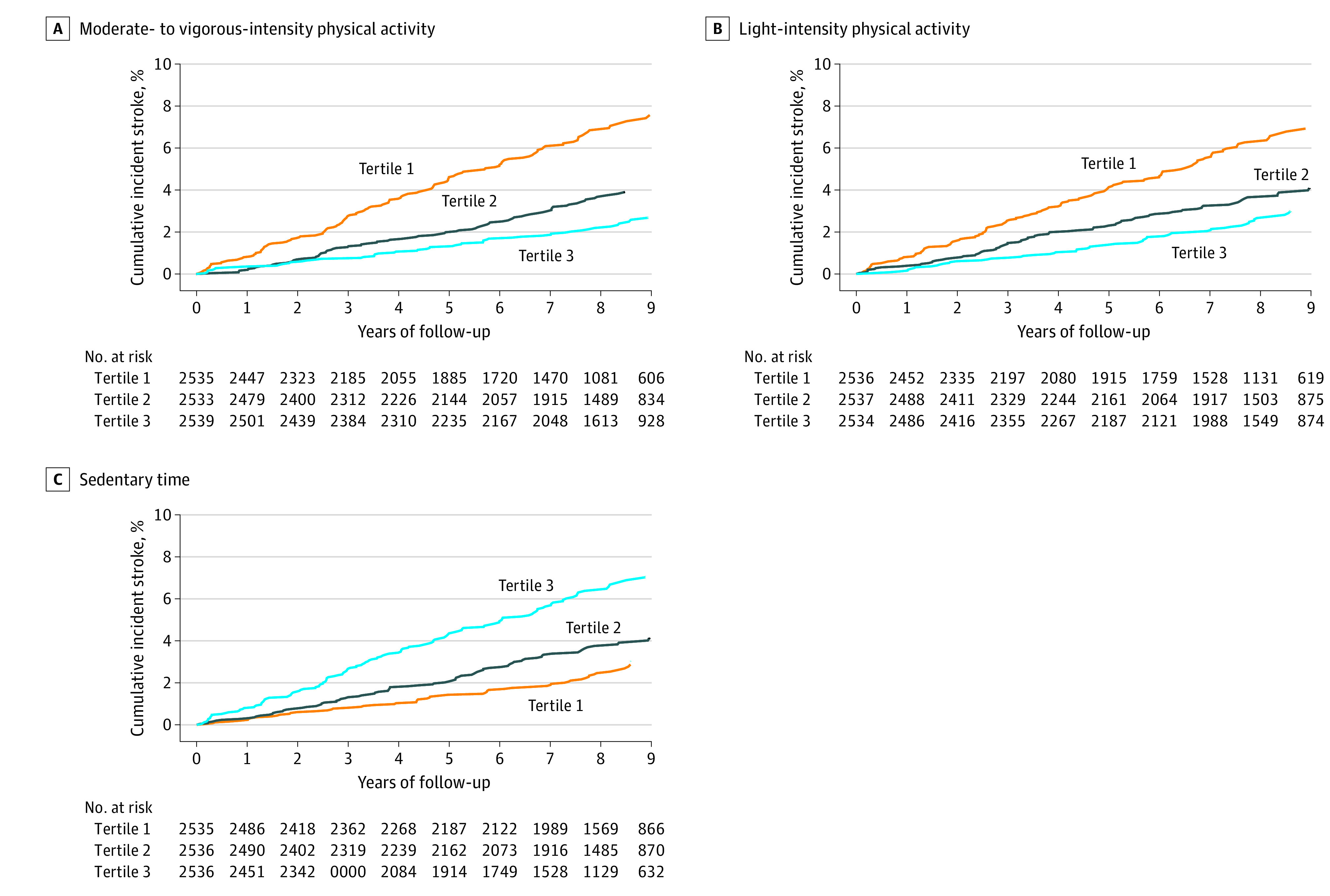
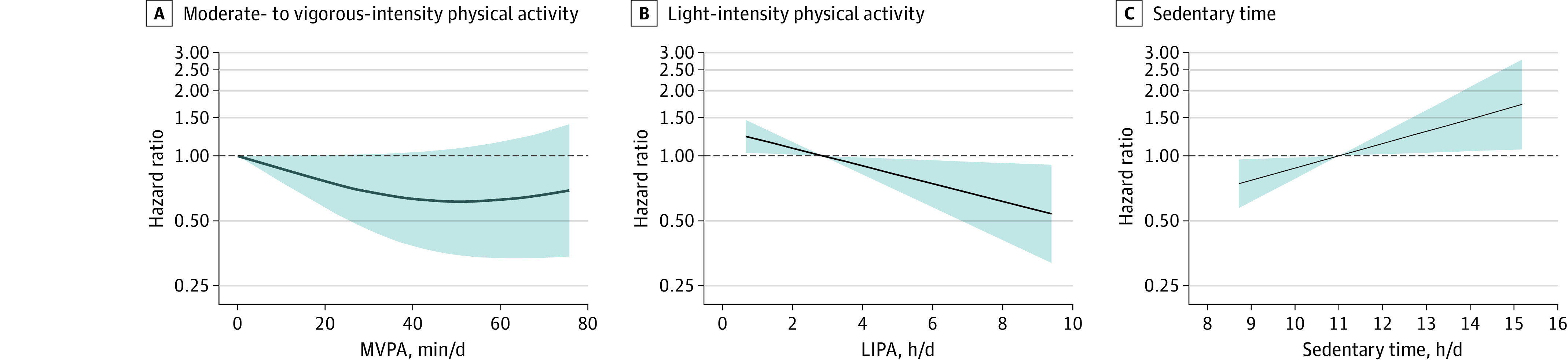
Among 7607 participants, the mean (SD) age was 63.4 (8.5) years; 4145 participants (54.5%) were female, 2407 (31.6%) were Black, and 5200 (68.4%) were White. A total of 2523 participants (33.2%) resided in the stroke belt, and 1638 (21.5%) resided in the stroke buckle. Over a mean (SD) of 7.4 (2.5) years of follow-up, 286 incident stroke cases (244 ischemic [85.3%]) occurred. The fully adjusted hazard ratios (HRs) for incident stroke in the highest tertile compared with the lowest tertile were 0.74 (95% CI, 0.53-1.04; P = .08) for LIPA and 0.57 (95% CI, 0.38-0.84; P = .004) for MVPA. Higher sedentary time was associated with a 44% greater risk of incident stroke (HR, 1.44; 95% CI, 0.99-2.07; P = .04). When comparing the highest with the lowest tertile, mean sedentary bout duration was associated with a significantly greater risk of incident stroke (HR, 1.53; 95% CI, 1.10-2.12; P = .008). After adjustment for sedentary time, the highest tertile of unbouted MVPA (shorter bouts [1-9 minutes]) was associated with a significantly lower risk of incident stroke compared with the lowest tertile (HR, 0.62; 95% CI, 0.41-0.94; P = .02); however, bouted MVPA (longer bouts [at least 10 minutes]) was not (HR, 0.78; 95% CI, 0.53-1.15; P = .17). When expressed as continuous variables, sedentary time was positively associated with incident stroke risk (HR per 1-hour/day increase in sedentary time: 1.14; 95% CI, 1.02-1.28; P = .02), and LIPA was negatively associated with incident stroke risk (HR per 1-hour/day increase in LIPA: 0.86; 95% CI, 0.77-0.97; P = .02).
In this cohort study, objectively measured LIPA, MVPA, and sedentary time were significantly and independently associated with incident stroke risk. Longer sedentary bout duration was also independently associated with an increased risk of incident stroke. These findings suggest that replacing sedentary time with LIPA, or even very short bouts of MVPA, may lower stroke risk, supporting the concept of moving more and sitting less as a beneficial stroke risk reduction strategy among adults.
由于之前依赖于自我报告的测量方法,因此仍需要充分确定预防中风所需的体力活动量和强度。此外,作为中风独立风险因素的客观测量的久坐时间与中风之间的关联尚不清楚。
研究加速度计测量的久坐时间以及不同强度和持续时间的体力活动与中风事件风险之间的关联。
设计、设置和参与者:本队列研究纳入了 Reasons for Geographic and Racial Differences in Stroke(REGARDS)研究的参与者,这些参与者于 2003 年 2 月 5 日至 2007 年 10 月 30 日入组。2009 年 5 月 12 日至 2013 年 1 月 5 日,美国大陆 45 岁及以上的 7607 名黑人和白人成年人收集了加速度计数据。由于科学和临床原因,没有收集其他种族和族裔的数据。出于设计目的,黑人和美国东南部中风带和中风扣的居民被过度抽样。数据于 2020 年 5 月 5 日至 2021 年 11 月 11 日进行分析。
久坐时间、低强度体力活动(LIPA)和中等到剧烈强度体力活动(MVPA)使用佩戴在臀部的加速度计测量,连续 7 天进行测量,并按三分位进行分析。
中风事件。
在 7607 名参与者中,平均(SD)年龄为 63.4(8.5)岁;4145 名参与者(54.5%)为女性,2407 名(31.6%)为黑人,5200 名(68.4%)为白人。共有 2523 名参与者(33.2%)居住在中风带,1638 名参与者(21.5%)居住在中风扣。在平均(SD)7.4(2.5)年的随访中,发生了 286 例中风事件(244 例缺血性[85.3%])。与最低三分位相比,最高三分位的全因调整后发生中风的风险比(HR)分别为 LIPA 的 0.74(95%CI,0.53-1.04;P=0.08)和 MVPA 的 0.57(95%CI,0.38-0.84;P=0.004)。久坐时间越高,中风事件的风险增加 44%(HR,1.44;95%CI,0.99-2.07;P=0.04)。与最低三分位相比,最高三分位的平均久坐时间与中风事件风险显著相关(HR,1.53;95%CI,1.10-2.12;P=0.008)。在调整久坐时间后,最高三分位的无间断 MVPA(较短的时间[1-9 分钟])与最低三分位相比,中风事件风险显著降低(HR,0.62;95%CI,0.41-0.94;P=0.02);然而,间断 MVPA(至少 10 分钟)则没有(HR,0.78;95%CI,0.53-1.15;P=0.17)。当以连续变量表示时,久坐时间与中风事件风险呈正相关(每增加 1 小时/天的静坐时间,HR 增加 1.14;95%CI,1.02-1.28;P=0.02),LIPA 与中风事件风险呈负相关(每增加 1 小时/天的 LIPA,HR 减少 0.86;95%CI,0.77-0.97;P=0.02)。
在这项队列研究中,客观测量的 LIPA、MVPA 和久坐时间与中风事件风险显著且独立相关。久坐时间的增加与中风事件风险的增加也独立相关。这些发现表明,用 LIPA 或甚至非常短的 MVPA 时间代替久坐时间可能会降低中风风险,支持成年人将更多的时间用于活动和减少久坐时间作为有益的中风风险降低策略的概念。