Department of Radiology and Nuclear Medicine, MS Center Amsterdam, Amsterdam Neuroscience, Amsterdam UMC, location VUmc, De Boelelaan 1118, 1081 HV Amsterdam PO box 7057, Amsterdam 1007 MB, The Netherlands.
Department of Radiology and Nuclear Medicine, MS Center Amsterdam, Amsterdam Neuroscience, Amsterdam UMC, location VUmc, De Boelelaan 1118, 1081 HV Amsterdam PO box 7057, Amsterdam 1007 MB, The Netherlands.
Neuroimage Clin. 2019;24:102074. doi: 10.1016/j.nicl.2019.102074. Epub 2019 Nov 5.
Accurate lesion segmentation is important for measurements of lesion load and atrophy in subjects with multiple sclerosis (MS). International MS lesion challenges show a preference of convolutional neural networks (CNN) strategies, such as nicMSlesions. However, since the software is trained on fairly homogenous training data, we aimed to test the performance of nicMSlesions in an independent dataset with manual and other automatic lesion segmentations to determine whether this method is suitable for larger, multi-center studies.
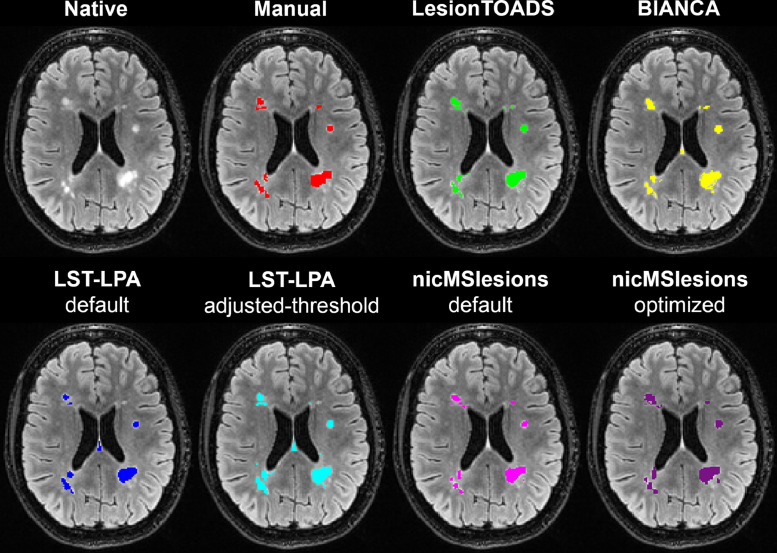
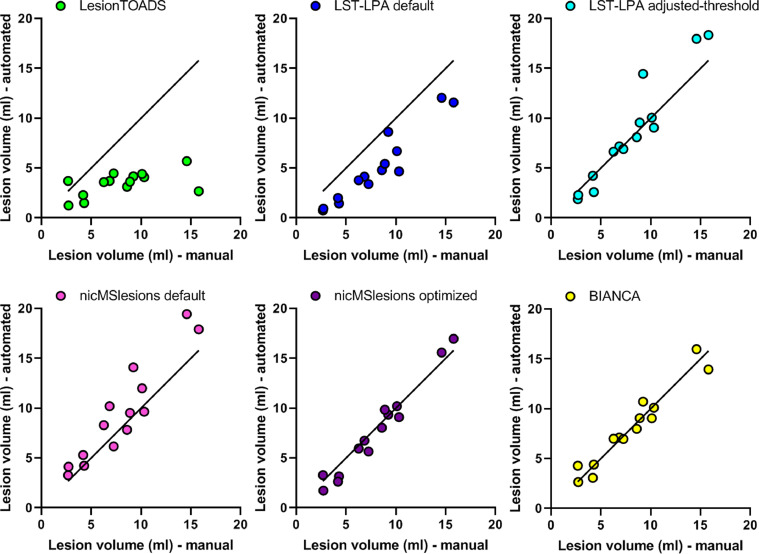
Manual lesion segmentation was performed in fourteen subjects with MS on sagittal 3D FLAIR images from a 3T GE whole-body scanner with 8-channel head coil. We compared five different categories of automated lesion segmentation methods for their volumetric and spatial agreement with manual segmentation: (i) unsupervised, untrained (LesionTOADS); (ii) supervised, untrained (LST-LPA and nicMSlesions with default settings); (iii) supervised, untrained with threshold adjustment (LST-LPA optimized for current data); (iv) supervised, trained with leave-one-out cross-validation on fourteen subjects with MS (nicMSlesions and BIANCA); and (v) supervised, trained on a single subject with MS (nicMSlesions). Volumetric accuracy was determined by the intra-class correlation coefficient (ICC) and spatial accuracy by Dice's similarity index (SI). Volumes and SI were compared between methods using repeated measures ANOVA or Friedman tests with post-hoc pairwise comparison.
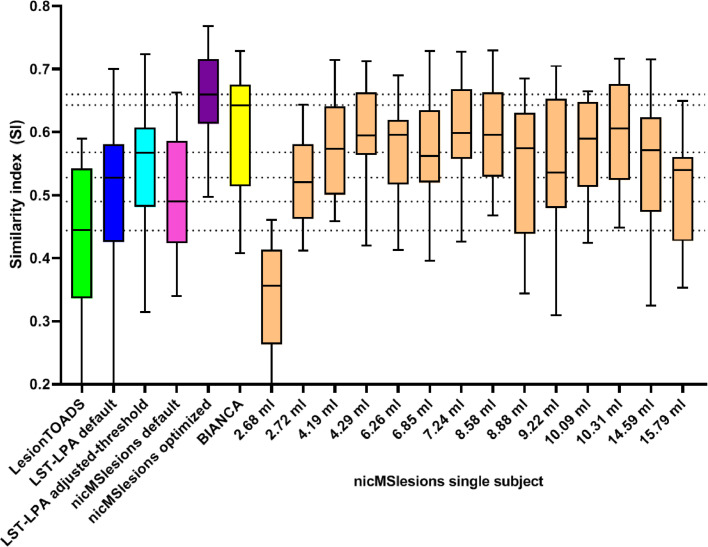
The best volumetric and spatial agreement with manual was obtained with the supervised and trained methods nicMSlesions and BIANCA (ICC absolute agreement > 0.968 and median SI > 0.643) and the worst with the unsupervised, untrained method LesionTOADS (ICC absolute agreement = 0.140 and median SI = 0.444). Agreement with manual in the single-subject network training of nicMSlesions was poor for input with low lesion volumes (i.e. two subjects with lesion volumes ≤ 3.0 ml). For the other twelve subjects, ICC varied from 0.593 to 0.973 and median SI varied from 0.535 to 0.606. In all cases, the single-subject trained nicMSlesions segmentations outperformed LesionTOADS, and in almost all cases it also outperformed LST-LPA.
Input from only one subject to re-train the deep learning CNN nicMSlesions is sufficient for adequate lesion segmentation, with on average higher volumetric and spatial agreement with manual than obtained with the untrained methods LesionTOADS and LST-LPA.
准确的病变分割对于多发性硬化症(MS)患者的病变负荷和萎缩测量非常重要。国际 MS 病变挑战赛倾向于使用卷积神经网络(CNN)策略,例如 nicMSlesions。然而,由于该软件是基于相当同质的训练数据进行训练的,我们旨在将 nicMSlesions 在一个独立的数据集上进行测试,该数据集具有手动和其他自动病变分割,以确定该方法是否适用于更大的、多中心的研究。
在 14 名 MS 患者的矢状位 3D FLAIR 图像上进行手动病变分割,这些图像来自 3T GE 全身扫描仪和 8 通道头部线圈。我们比较了五种不同类别的自动病变分割方法在体积和空间上与手动分割的一致性:(i)无监督、未训练(LesionTOADS);(ii)有监督、未训练(LST-LPA 和默认设置下的 nicMSlesions);(iii)有监督、未训练但阈值调整(针对当前数据优化的 LST-LPA);(iv)在 14 名 MS 患者上进行了基于留一交叉验证的有监督、训练(nicMSlesions 和 BIANCA);和(v)在单个 MS 患者上进行了有监督、训练(nicMSlesions)。体积准确性通过组内相关系数(ICC)确定,空间准确性通过 Dice 相似性指数(SI)确定。使用重复测量方差分析或 Friedman 检验,对各种方法之间的体积和 SI 进行比较,并进行事后两两比较。
与手动方法最一致的是有监督和训练的方法 nicMSlesions 和 BIANCA(ICC 绝对一致性>0.968,中位数 SI>0.643),而最不一致的是无监督、未训练的方法 LesionTOADS(ICC 绝对一致性=0.140,中位数 SI=0.444)。在单个患者网络训练中,nicMSlesions 的输入病变体积较低时(即两名患者的病变体积≤3.0ml),与手动方法的一致性较差。对于其他 12 名患者,ICC 从 0.593 到 0.973,中位数 SI 从 0.535 到 0.606。在所有情况下,单个患者训练的 nicMSlesions 分割都优于 LesionTOADS,并且在几乎所有情况下,它也优于 LST-LPA。
仅从一个患者输入重新训练深度学习 CNN nicMSlesions 就足以进行充分的病变分割,与未经训练的方法 LesionTOADS 和 LST-LPA 相比,平均具有更高的体积和空间一致性。