Sanger Heart and Vascular Institute, Atrium Health, Charlotte, NC, USA.
Department of Cardiology, Kaiser Permanente San Francisco Medical Center, San Francisco, CA, USA.
Eur J Heart Fail. 2020 Jul;22(7):1174-1182. doi: 10.1002/ejhf.1659. Epub 2019 Dec 21.
Worsening heart failure (HF) is associated with shorter left ventricular systolic ejection time (SET), but there are limited data describing the relationship between SET and clinical outcomes. Thus, the objective was to describe the association between SET and clinical outcomes in an ambulatory HF population irrespective of ejection fraction (EF).
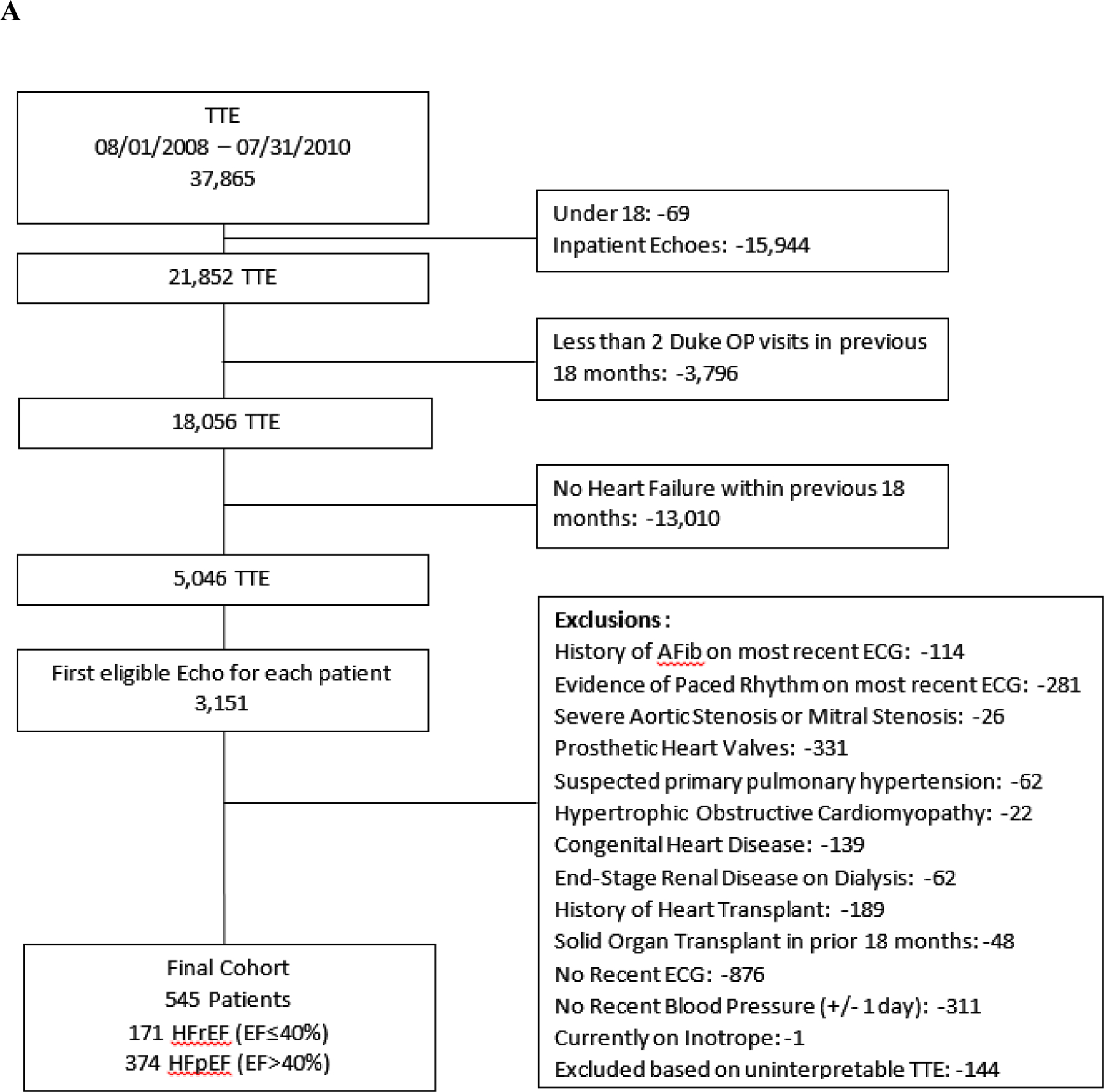
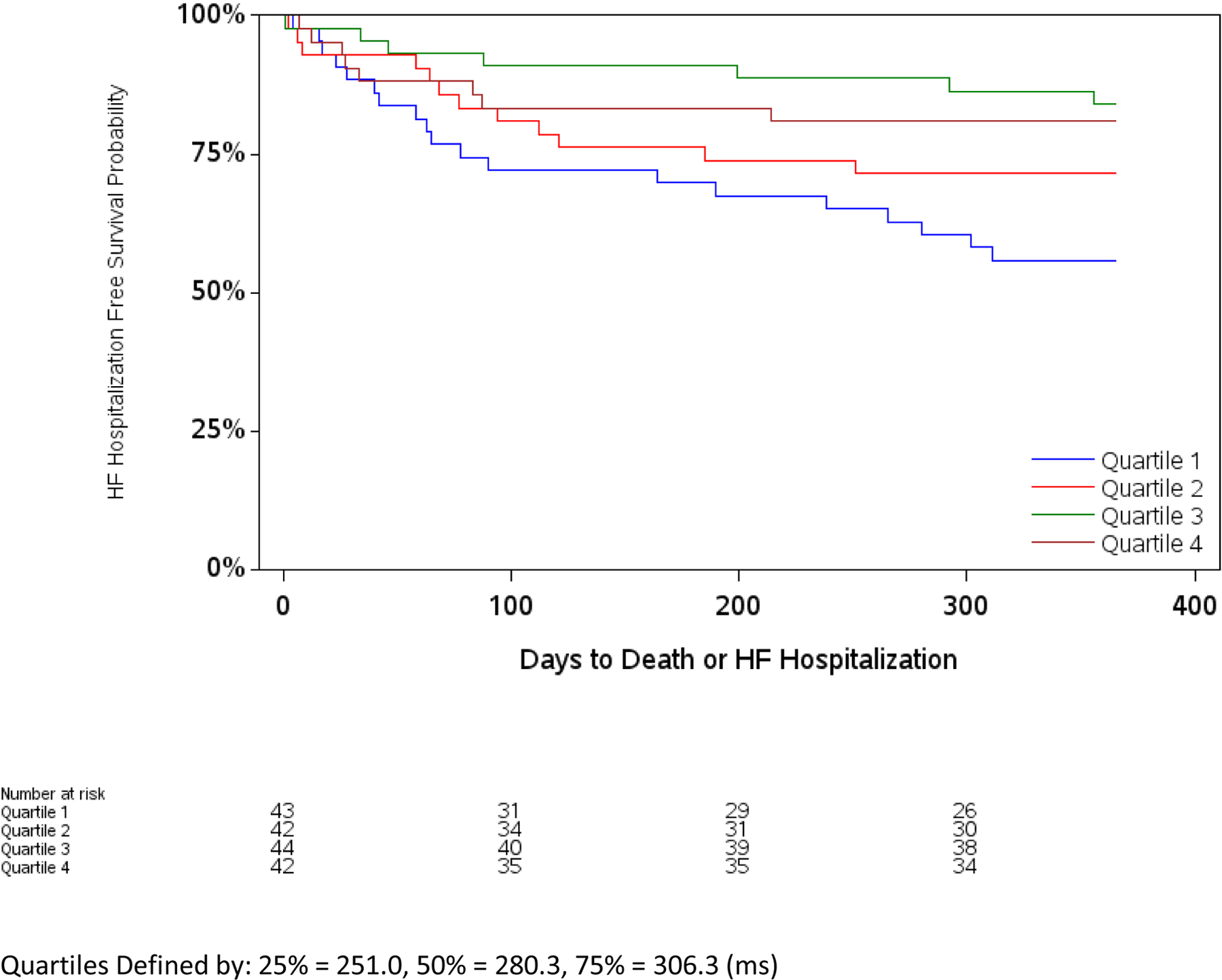
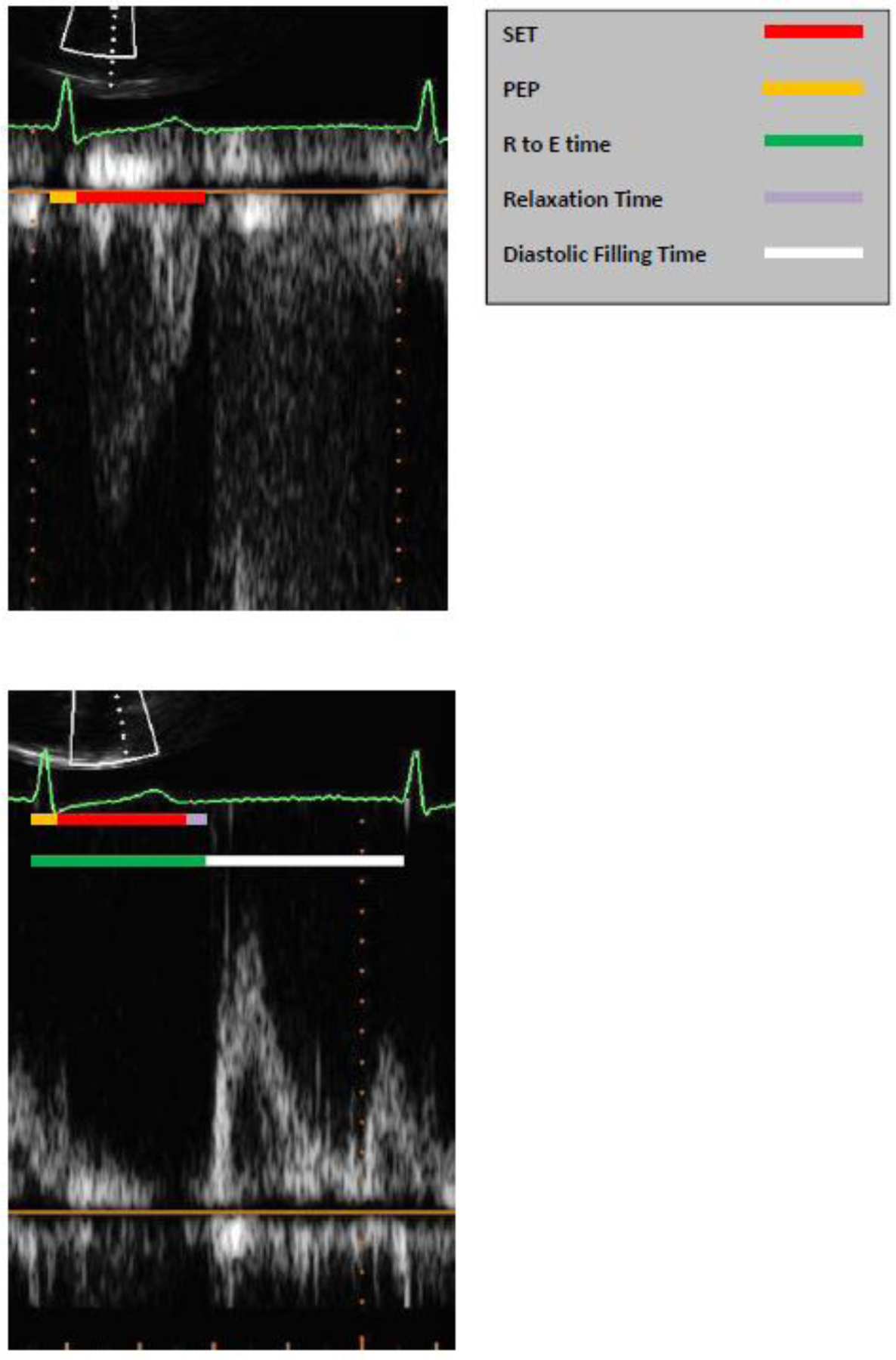
We identified ambulatory patients with HF with reduced EF (HFrEF) and HF with preserved EF (HFpEF) who had an outpatient transthoracic echocardiogram performed between August 2008 and July 2010 at a tertiary referral centre. Multivariable logistic regression was used to evaluate the association between SET and 1-year outcomes. A total of 545 HF patients (171 HFrEF, 374 HFpEF) met eligibility criteria. Compared with HFpEF, HFrEF patients were younger [median age 60 years (25th-75th percentiles 50-69) vs. 64 years (25th-75th percentiles 53-74], with fewer females (30% vs. 56%) and a similar percentage of African Americans (36% vs. 35%). Median (25th-75th percentiles) EF with HFrEF was 30% (25-35%) and with HFpEF was 54% (48-58%). Median SET was shorter (280 ms vs. 315 ms, P < 0.001), median pre-ejection period was longer (114 ms vs. 89 ms, P < 0.001), and median relaxation time was shorter (78.7 ms vs. 93.3 ms, P < 0.001) among patients with HFrEF vs. HFpEF. Death or HF hospitalization occurred in 26.9% (n = 46) HFrEF and 11.8% (n = 44) HFpEF patients. After adjustment, longer SET was associated with lower odds of the composite of death or HF hospitalization at 1 year among HFrEF but not HFpEF patients.
Longer SET is independently associated with improved outcomes among HFrEF patients but not HFpEF patients, supporting a potential role for normalizing SET as a therapeutic strategy with systolic dysfunction.
心力衰竭(HF)恶化与左心室收缩射血时间(SET)缩短有关,但描述 SET 与临床结局之间关系的数据有限。因此,本研究旨在描述门诊 HF 人群中,无论射血分数(EF)如何,SET 与临床结局之间的关系。
我们在一家三级转诊中心,于 2008 年 8 月至 2010 年 7 月期间,识别出了 EF 降低的心力衰竭(HFrEF)和 EF 保留的心力衰竭(HFpEF)的门诊 HF 患者,并对其进行了经胸超声心动图检查。多变量逻辑回归用于评估 SET 与 1 年结局之间的关系。共有 545 名 HF 患者(HFrEF 患者 171 名,HFpEF 患者 374 名)符合入选标准。与 HFpEF 患者相比,HFrEF 患者更年轻[中位年龄 60 岁(25 至 75 百分位数为 50 至 69)比 64 岁(25 至 75 百分位数为 53 至 74)],女性比例较少(30%比 56%),非裔美国人比例相似(36%比 35%)。HFrEF 患者的中位(25 至 75 百分位数)EF 为 30%(25%至 35%),HFpEF 患者的中位 EF 为 54%(48%至 58%)。HFrEF 患者的中位 SET 较短(280 毫秒比 315 毫秒,P<0.001),中位射前间期较长(114 毫秒比 89 毫秒,P<0.001),中位舒张时间较短(78.7 毫秒比 93.3 毫秒,P<0.001)。HFrEF 患者中有 26.9%(n=46)死亡或 HF 住院,HFpEF 患者中有 11.8%(n=44)死亡或 HF 住院。调整后,在 HFrEF 患者中,较长的 SET 与 1 年时死亡或 HF 住院的复合终点的可能性降低相关,但在 HFpEF 患者中则无此相关性。
在 HFrEF 患者中,较长的 SET 与改善结局独立相关,但在 HFpEF 患者中则无此相关性,这支持将 SET 正常化作为治疗收缩功能障碍的一种潜在治疗策略。