Narayan Snaiha I, Terre Giselle V, Amin Rutvi, Shanghavi Keshvi V, Chandrashekar Gayathri, Ghouse Farhana, Ahmad Binish A, S Gowri N, Satram Christena, Majid Hamna A, Bayoro Danielle K
Department of Medicine, Trinity College Dublin, Dublin, IRL.
Department of Medicine, Universidad Iberoamericana (UNIBE), Santo Domingo, DOM.
Cureus. 2023 Sep 21;15(9):e45719. doi: 10.7759/cureus.45719. eCollection 2023 Sep.
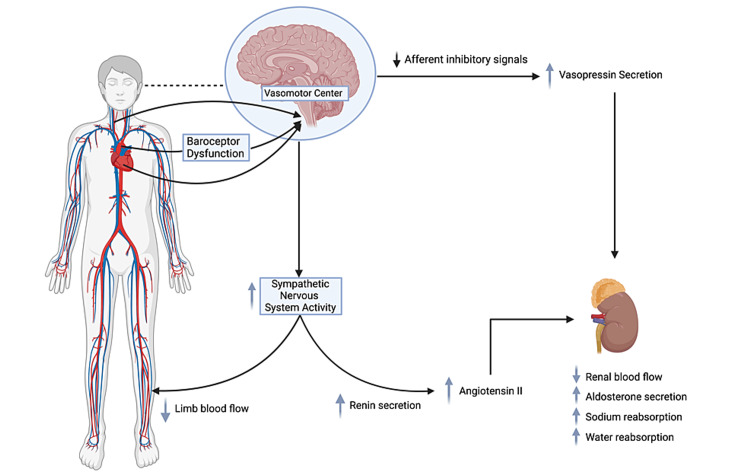
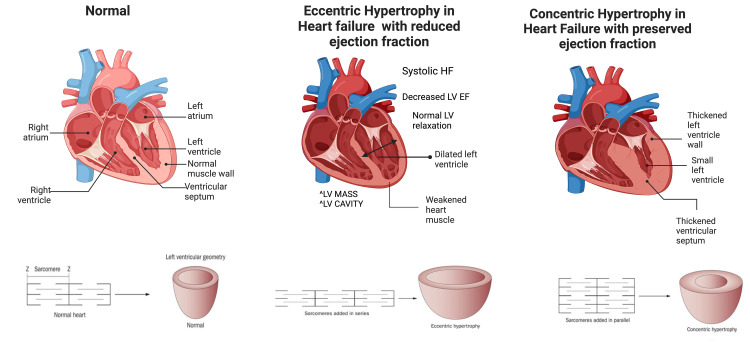
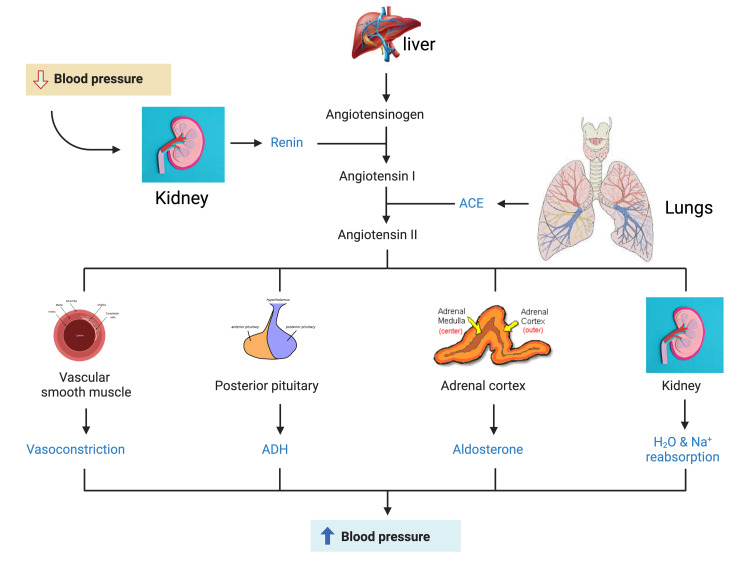
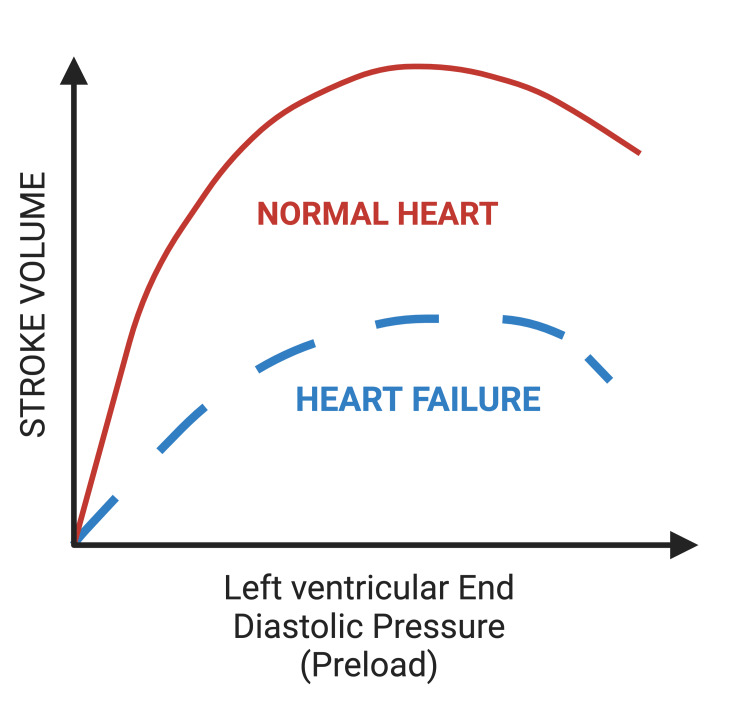
Heart failure with reduced ejection fraction (HFrEF) is a clinical syndrome whose management has significantly evolved based on the pathophysiology and disease process. It is widely prevalent, has a relatively high mortality rate, and is comparatively more common in men than women. In HFrEF, the series of maladaptive processes that occur lead to an inability of the muscle of the left ventricle to pump blood efficiently and effectively, causing cardiac dysfunction. The neurohormonal and hemodynamic adaptations play a significant role in the advancement of the disease and are critical to guiding the treatment and management of HFrEF. The first-line therapy, which includes loop diuretics, β-blockers, angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers, hydralazine/isosorbide-dinitrate, and mineralocorticoid receptor antagonists (MRAs), has been proven to provide symptomatic relief and decrease mortality and complications. The newly recommended drugs for guideline-based therapy, angiotensin receptor/neprilysin inhibitor (ARNI), sodium-glucose cotransporter 2 inhibitors, soluble guanylate cyclase, and myosin activators and modulators have also been shown to improve cardiac function, reverse cardiac remodeling, and reduce mortality rates. Recent studies have demonstrated that exercise-based therapy has resulted in an improved quality of life, exercise capacity, cardiac function, and decreased hospital readmission rates, but it has not had a considerable reduction in mortality rates. Combining multiple therapies alongside holistic advances such as exercise therapy may provide synergistic benefits, ultimately leading to improved outcomes for patients with HFrEF. Although first-line treatment, novel pharmacologic management, and exercise-based therapy have been shown to improve prognosis, the existing literature suggests a need for further studies evaluating the long-term effects of MRA and ARNI.
射血分数降低的心力衰竭(HFrEF)是一种临床综合征,其管理已根据病理生理学和疾病进程有了显著进展。它广泛流行,死亡率相对较高,且在男性中比女性更为常见。在HFrEF中,发生的一系列适应不良过程导致左心室肌肉无法有效地泵血,从而引起心脏功能障碍。神经激素和血流动力学适应在疾病进展中起重要作用,对指导HFrEF的治疗和管理至关重要。一线治疗包括袢利尿剂、β受体阻滞剂、血管紧张素转换酶抑制剂/血管紧张素II受体阻滞剂、肼屈嗪/硝酸异山梨酯和盐皮质激素受体拮抗剂(MRAs),已被证明可缓解症状并降低死亡率和并发症。基于指南的治疗新推荐药物,血管紧张素受体/脑啡肽酶抑制剂(ARNI)、钠-葡萄糖协同转运蛋白2抑制剂、可溶性鸟苷酸环化酶、肌球蛋白激活剂和调节剂也已显示可改善心脏功能、逆转心脏重塑并降低死亡率。最近的研究表明,基于运动的治疗可改善生活质量、运动能力、心脏功能并降低住院再入院率,但对死亡率的降低作用并不显著。将多种治疗与运动疗法等整体进展相结合可能会产生协同效益,最终改善HFrEF患者的预后。尽管一线治疗、新型药物管理和基于运动的治疗已显示可改善预后,但现有文献表明需要进一步研究评估MRA和ARNI的长期效果。