Department of Cardiovascular Surgery, Nihon University, Itabashi-ku, Tokyo, Japan.
Department of Cardiovascular Surgery, Saitama Medical Center, Jichi Medical University, Omiya-ku, Saitama, Japan.
PLoS One. 2020 Feb 6;15(2):e0228954. doi: 10.1371/journal.pone.0228954. eCollection 2020.
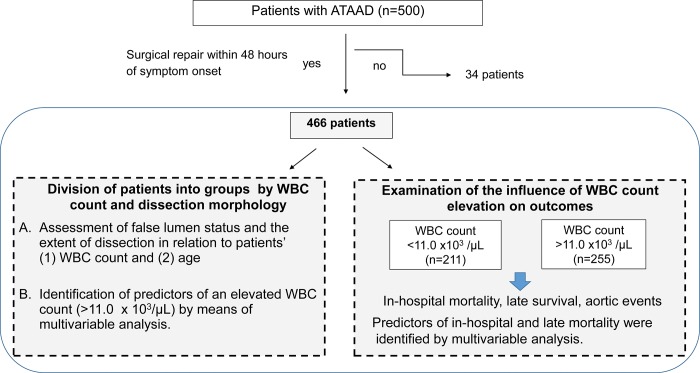
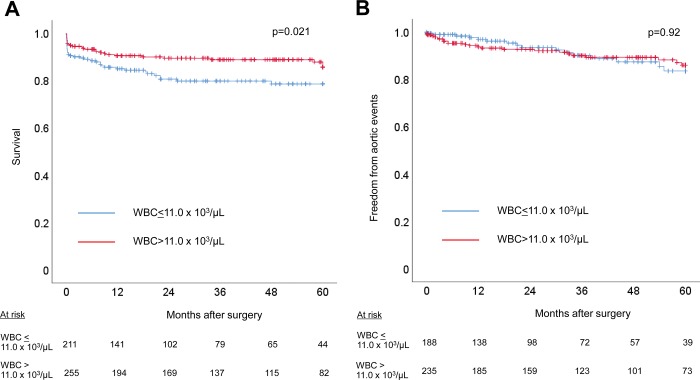
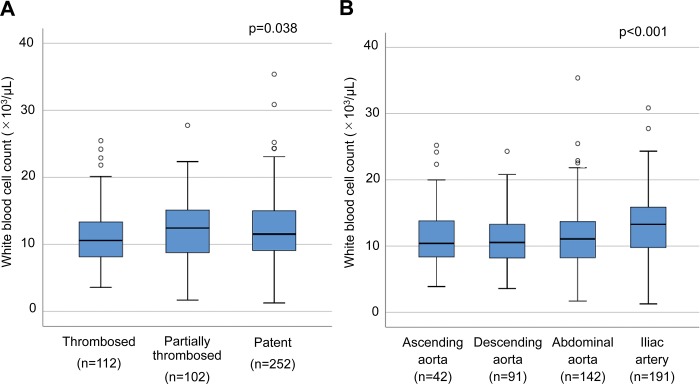
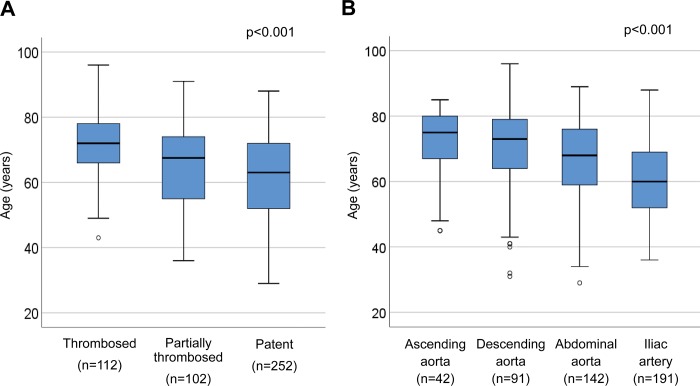
Aortic dissection may induce a systemic inflammatory reaction. The etiological backgrounds for elevation of the white blood cell count remain to be clarified. In 466 patients with acute type A aortic dissection treated surgically within 48 hours of symptom onset, the etiologic background of an elevated admission white blood cell count and the effect of such elevation on outcomes were assessed retrospectively. Patients' white blood cell count differed significantly in relation to the extent of dissection, with a median (25th, 75th percentile) white blood cell count of 10.4 (8.1, 13.9) x 103/μL for dissection confined to the ascending aorta, 10.5 (8.2,13.) 103/μL for dissection extending to the aortic arch/descending aorta, 11.1 (8.2, 13.7) x 103/μL for extension to the abdominal aorta, and 13.3 (9.8, 15.9) x 103/μL for extension to the iliac artery (p<0.001). With 11.0 x 103/μL used as the cut-off value for white blood cell count elevation, multivariable analysis showed current smoking (p<0.001; odds ratio, 2.79), dissection extending to the iliac artery (p = 0.006; odds ratio, 1.79), age (p = 0.007, odds ratio, 0.98), and no coronary ischemia (p = 0.027, odds ratio, 2.22) to be factors related to the elevated white blood cell count. Mean age differed significantly between patients with and without an elevated white blood cell count (62.3 vs. 68.3 years, p <0.001). Although in-hospital mortality was similar (7.5% vs.10.9%, p = 0.19), 5-year survival was lower in patients without an elevated count (85.7% vs. 78.6%, p = 0.019), reflecting their more advanced age. In conclusion, our data suggest that dissection morphology and patient age influence the acute phase systemic inflammatory response associated with an elevated white blood cell count in patients with ATAAD. A better understanding of this relation may help optimize diagnosis and perioperative care.
升主动脉夹层可能会引发全身性炎症反应。白细胞计数升高的病因背景仍有待阐明。在 466 例在发病后 48 小时内接受手术治疗的急性 A 型主动脉夹层患者中,回顾性评估了入院时白细胞计数升高的病因背景及其对预后的影响。患者的白细胞计数与夹层的范围明显相关,局限于升主动脉夹层的患者的中位(25 百分位,75 百分位)白细胞计数为 10.4(8.1,13.9)×103/μL,升主动脉夹层扩展至主动脉弓/降主动脉的患者为 10.5(8.2,13.0)×103/μL,升主动脉夹层扩展至腹主动脉的患者为 11.1(8.2,13.7)×103/μL,升主动脉夹层扩展至髂动脉的患者为 13.3(9.8,15.9)×103/μL(p<0.001)。以 11.0×103/μL 作为白细胞计数升高的截断值,多变量分析显示,当前吸烟(p<0.001;比值比,2.79)、髂动脉夹层延伸(p=0.006;比值比,1.79)、年龄(p=0.007,比值比,0.98)和无冠状动脉缺血(p=0.027,比值比,2.22)是与白细胞计数升高相关的因素。白细胞计数升高和不升高的患者的平均年龄差异有统计学意义(62.3 岁 vs. 68.3 岁,p<0.001)。虽然住院死亡率相似(7.5% vs. 10.9%,p=0.19),但白细胞计数不升高的患者 5 年生存率较低(85.7% vs. 78.6%,p=0.019),反映出他们的年龄较大。总之,我们的数据表明,在 ATAAD 患者中,夹层形态和患者年龄影响与白细胞计数升高相关的急性期全身炎症反应。更好地了解这种关系可能有助于优化诊断和围手术期护理。