Division of Cardiology, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Republic of Korea.
Cardiovascular Center, Division of Cardiology, Seoul National University Bundang Hospital, Seongnam, Republic of Korea.
BMJ Open. 2020 Feb 6;10(2):e030514. doi: 10.1136/bmjopen-2019-030514.
Guideline-directed medical therapy (GDMT) with renin-angiotensin system (RAS) inhibitors and beta-blockers has improved survival in patients with heart failure with reduced ejection fraction (HFrEF). As clinical trials usually do not include very old patients, it is unknown whether the results from clinical trials are applicable to elderly patients with HF. This study was performed to investigate the clinical characteristics and treatment strategies for elderly patients with HFrEF in a large prospective cohort.
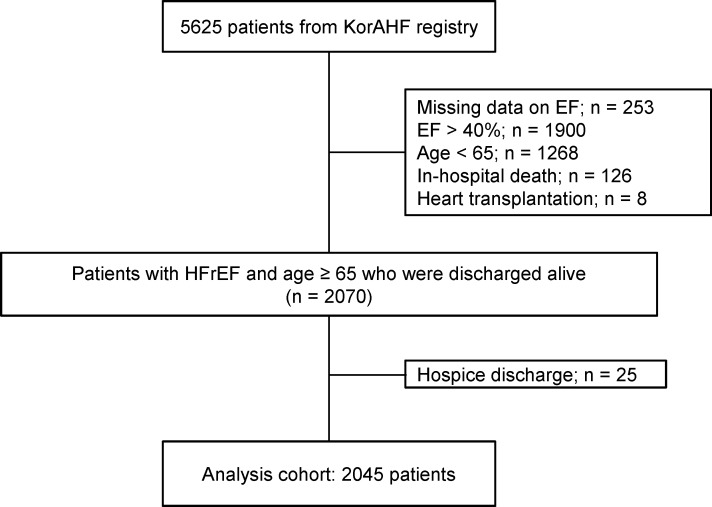
The Korean Acute Heart Failure (KorAHF) registry consecutively enrolled 5625 patients hospitalised for acute HF from 10 tertiary university hospitals in Korea.
In this study, 2045 patients with HFrEF who were aged 65 years or older were included from the KorAHF registry.
All-cause mortality data were obtained from medical records, national insurance data or national death records.
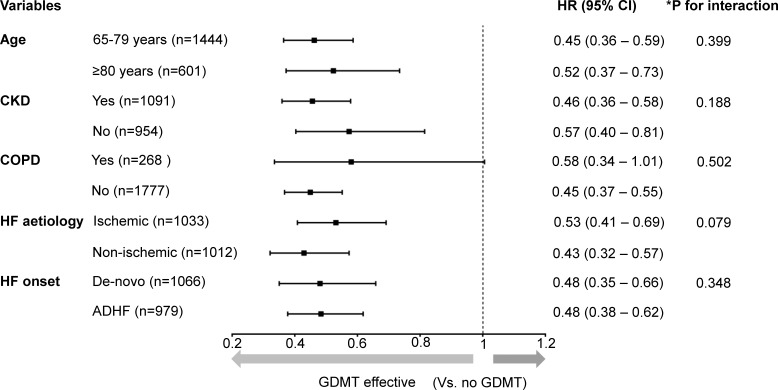
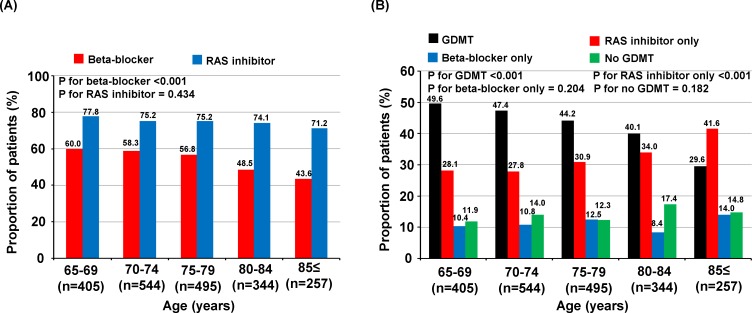
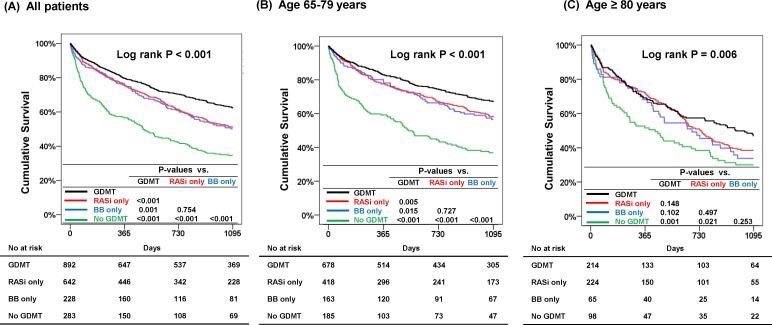
Both beta-blockers and RAS inhibitors were used in 892 (43.8%) patients (GDMT group), beta-blockers only in 228 (11.1%) patients, RAS inhibitors only in 642 (31.5%) patients and neither beta-blockers nor RAS inhibitors in 283 (13.6%) patients (no GDMT group). With increasing age, the GDMT rate decreased, which was mainly attributed to the decreased prescription of beta-blockers. In multivariate analysis, GDMT was associated with a 53% reduced risk of all-cause mortality (HR 0.47, 95% CI 0.39 to 0.57) compared with no GDMT. Use of beta-blockers only (HR 0.57, 95% CI 0.45 to 0.73) and RAS inhibitors only (HR 0.58, 95% CI 0.48 to 0.71) was also associated with reduced risk. In a subgroup of very elderly patients (aged ≥80 years), the GDMT group had the lowest mortality.
GDMT was associated with reduced 3-year all-cause mortality in elderly and very elderly HFrEF patients.
NCT01389843.
指南指导的医学治疗(GDMT)联合肾素-血管紧张素系统(RAS)抑制剂和β受体阻滞剂可改善射血分数降低的心力衰竭(HFrEF)患者的生存率。由于临床试验通常不包括非常高龄的患者,因此尚不清楚临床试验的结果是否适用于老年 HF 患者。本研究旨在调查大型前瞻性队列中年龄较大的 HFrEF 患者的临床特征和治疗策略。
韩国急性心力衰竭(KorAHF)登记处连续纳入了来自韩国 10 家三级大学医院的因急性 HF 住院的 5625 例患者。
本研究从 KorAHF 登记处纳入了 2045 例年龄在 65 岁或以上的 HFrEF 患者。
所有原因死亡率数据均从病历、国家保险数据或国家死亡记录中获得。
β受体阻滞剂和 RAS 抑制剂均使用(GDMT 组)的患者有 892 例(43.8%),仅使用β受体阻滞剂的患者有 228 例(11.1%),仅使用 RAS 抑制剂的患者有 642 例(31.5%),既未使用β受体阻滞剂也未使用 RAS 抑制剂的患者有 283 例(13.6%)(无 GDMT 组)。随着年龄的增加,GDMT 率下降,这主要归因于β受体阻滞剂的处方减少。多变量分析显示,与无 GDMT 相比,GDMT 使全因死亡率降低 53%(HR 0.47,95%CI 0.39 至 0.57)。仅使用β受体阻滞剂(HR 0.57,95%CI 0.45 至 0.73)和仅使用 RAS 抑制剂(HR 0.58,95%CI 0.48 至 0.71)也与风险降低相关。在非常高龄患者(年龄≥80 岁)亚组中,GDMT 组死亡率最低。
GDMT 可降低老年和非常高龄 HFrEF 患者的 3 年全因死亡率。
NCT01389843。