Khoury College of Computer Sciences, Northeastern University, 440 Huntington Ave, Boston, MA, 02115, USA.
Department of Civil & Environmental Engineering, Tufts University, Medford, MA, USA.
Environ Health. 2020 Feb 17;19(1):20. doi: 10.1186/s12940-020-00575-0.
The shape of the exposure-response curve for long-term ambient fine particulate (PM) exposure and cause-specific mortality is poorly understood, especially for rural populations and underrepresented minorities.
We used hybrid machine learning and Cox proportional hazard models to assess the association of long-term PM exposures on specific causes of death for 53 million U.S. Medicare beneficiaries (aged ≥65) from 2000 to 2008. Models included strata for age, sex, race, and ZIP code and controlled for neighborhood socio-economic status (SES) in our main analyses, with approximately 4 billion person-months of follow-up, and additionally for warm season average of 1-h daily maximum ozone exposures in a sensitivity analysis. The impact of non-traffic PM on mortality was examined using two stage models of PM and nitrogen dioxide (NO).
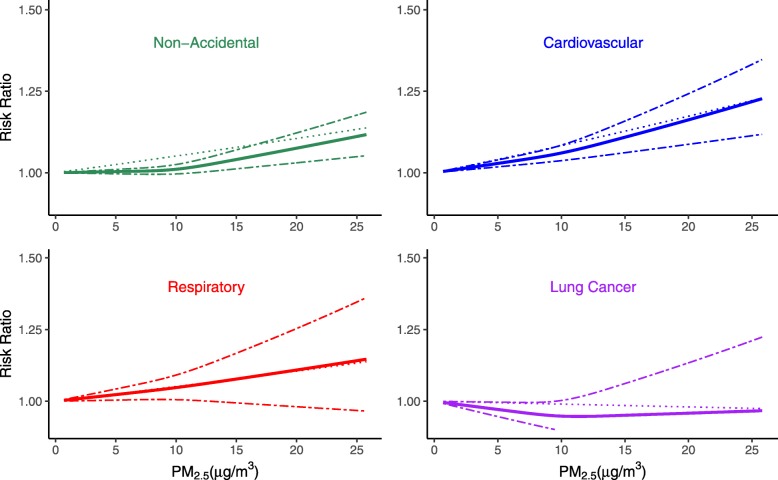
A 10 μg /m increase in 12-month average PM prior to death was associated with a 5% increase in all-cause mortality, as well as an 8.8, 5.6, and 2.5% increase in all cardiovascular disease (CVD)-, all respiratory-, and all cancer deaths, respectively, in age, gender, race, ZIP code, and SES-adjusted models. PM exposures, however, were not associated with lung cancer mortality. Results were not sensitive to control for ozone exposures. PM-mortality associations for CVD- and respiratory-related causes were positive and significant for beneficiaries irrespective of their sex, race, age, SES and urbanicity, with no evidence of a lower threshold for response or of lower Risk Ratios (RRs) at low PM levels. Associations between PM and CVD and respiratory mortality were linear and were higher for younger, Black and urban beneficiaries, but were largely similar by SES. Risks associated with non-traffic PM were lower than that for all PM and were null for respiratory and lung cancer-related deaths.
PM was associated with mortality from CVD, respiratory, and all cancer, but not lung cancer. PM-associated risks of CVD and respiratory mortality were similar across PM levels, with no evidence of a threshold. Blacks, urban, and younger beneficiaries were most vulnerable to the long-term impacts of PM on mortality.
长期暴露于细颗粒物(PM)与特定死因之间的关系的暴露-反应曲线形状尚不清楚,特别是对于农村人口和代表性不足的少数族裔。
我们使用混合机器学习和 Cox 比例风险模型,评估了 2000 年至 2008 年期间,5300 万美国医疗保险受益人(年龄≥65 岁)的长期 PM 暴露与特定死因之间的关联。模型包括年龄、性别、种族和邮政编码的分层,并在主要分析中控制了邻里社会经济地位(SES),随访时间约为 40 亿人月,在敏感性分析中还控制了温暖季节 1 小时每日最大臭氧暴露的平均水平。使用 PM 和二氧化氮(NO)的两阶段模型来检验非交通 PM 对死亡率的影响。
死亡前 12 个月 PM 的 10μg/m 增加与全因死亡率增加 5%相关,分别与所有心血管疾病(CVD)、所有呼吸系统疾病和所有癌症死亡率增加 8.8%、5.6%和 2.5%相关,在年龄、性别、种族、邮政编码和 SES 调整模型中。然而,PM 暴露与肺癌死亡率无关。结果不受臭氧暴露的控制影响。对于 CVD 和呼吸系统相关原因,PM 死亡率的相关性在无论其性别、种族、年龄、SES 和城市程度如何的受益人中均为阳性且显著,没有反应的下限或低 PM 水平下的风险比(RR)较低的证据。PM 与 CVD 和呼吸死亡率之间的关联呈线性,对于年轻、黑人受益人和城市受益人的关联更高,但 SES 差异不大。与非交通 PM 相关的风险低于所有 PM,与呼吸系统和肺癌相关的死亡无关。
PM 与 CVD、呼吸和所有癌症的死亡率相关,但与肺癌无关。PM 与 CVD 和呼吸死亡率之间的相关性在 PM 水平相似,没有证据表明存在阈值。黑人、城市和年轻的受益人群最容易受到 PM 对死亡率的长期影响。