Soral Merve, Altun Gülbin Töre, Dinçer Pelin Çorman, Arslantaş Mustafa Kemal, Aykaç Zuhal
Kastamonu State Hospital, Kastamonu, Turkey.
Department of Anaesthesiology and Reanimation, Marmara University Pendik Training and Research Hospital, İstanbul, Turkey.
Turk J Anaesthesiol Reanim. 2020 Feb;48(1):50-57. doi: 10.5152/TJAR.2019.45077. Epub 2019 Sep 24.
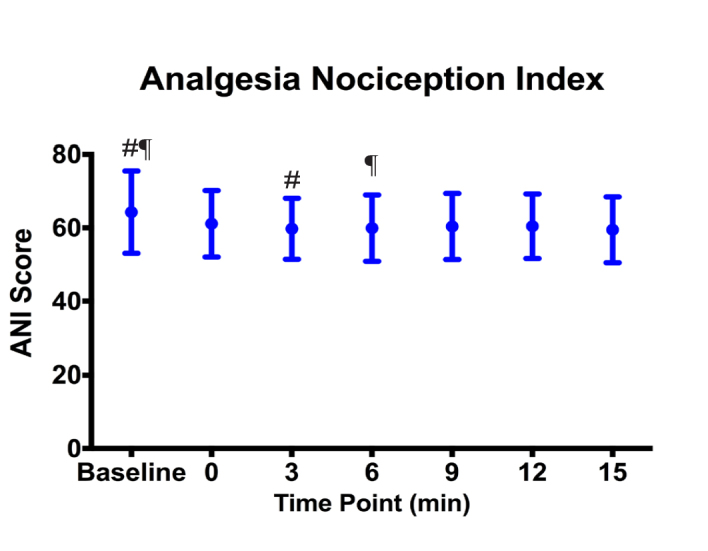
The objective of this study was to improve the patient comfort and safety during procedures done under anaesthesia and sedation. The analgesia nociception index (ANI) noninvasively provides information on the nociception-antinociception balance, and it can be used to assess analgesia objectively. We aimed to compare the effects of analgesia management with conventional methods and with ANI monitoring on total opioid consumption, sedation and analgesia levels in patients who underwent colonoscopy using sedo-analgesia.
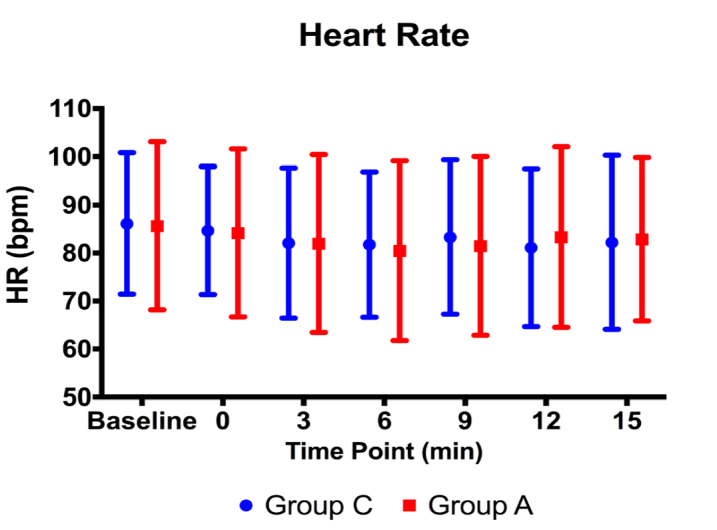
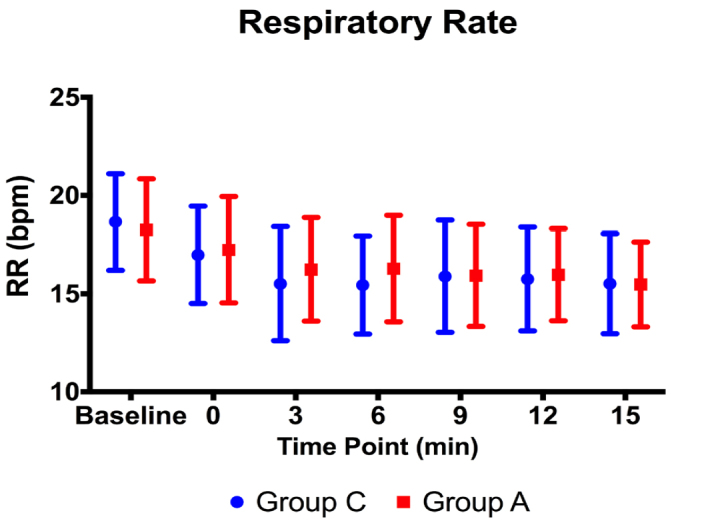
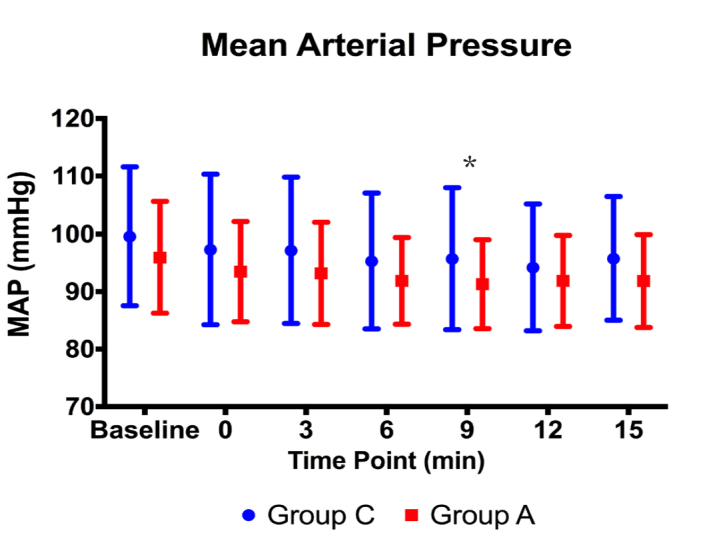
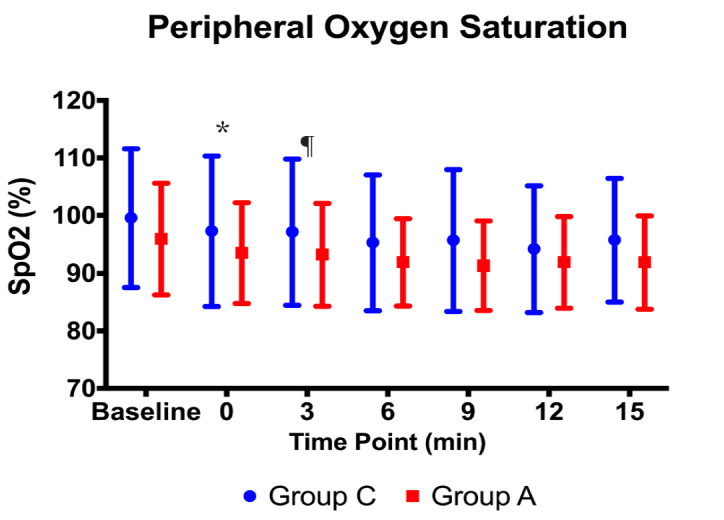
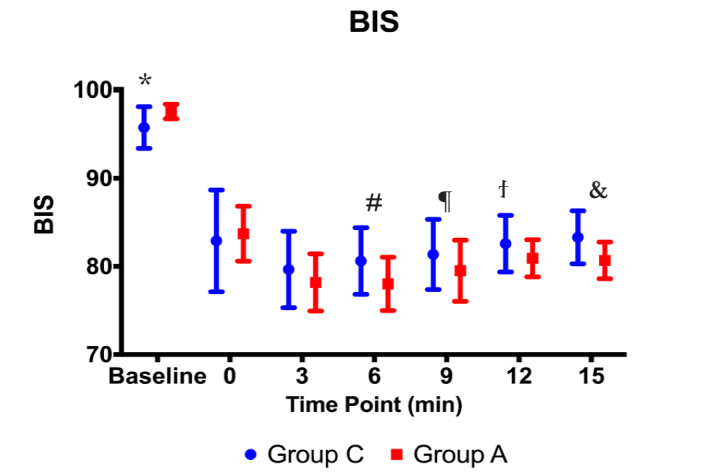
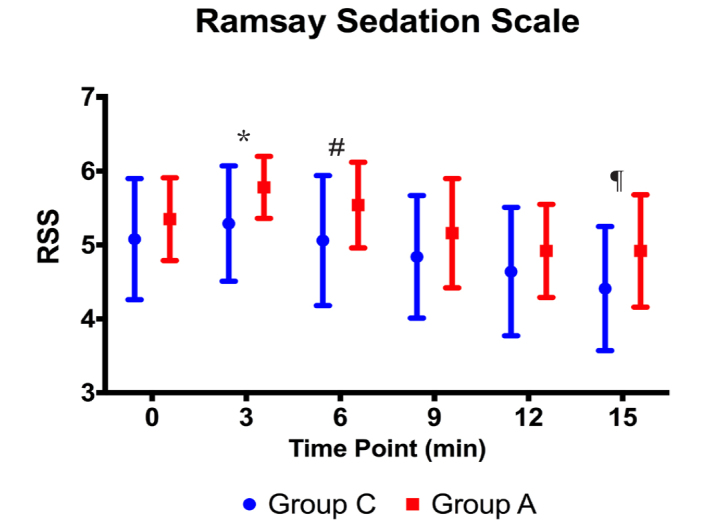
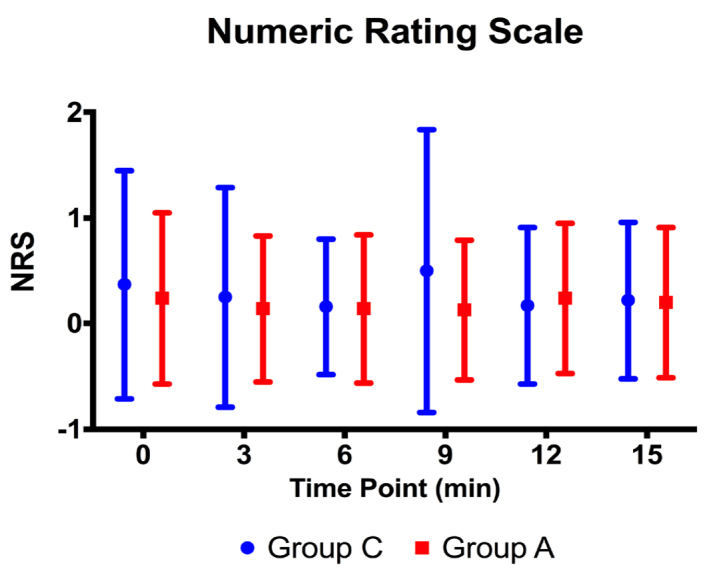
Adult patients (n=102), scheduled for procedural sedation, were prospectively analysed. After the induction with propofol and ketamine, infusions of propofol (2 mg kg h) and remifentanil (0.05 mcg kg min) were started. In Group A, remifentanil infusions were titrated to maintain the ANI value between 50 and 70, whereas in Group C, analgesic requirements were met according to the attending anaesthetist's intention. The heart rate, blood pressure, respiratory rate, SpO, BIS, Numeric Rating Scale (NRS) and Ramsay Sedation Scale were monitored. Complications, analgesics consumption, duration of the procedure, demographic information, NRS and the Modified Aldrete Score were evaluated.
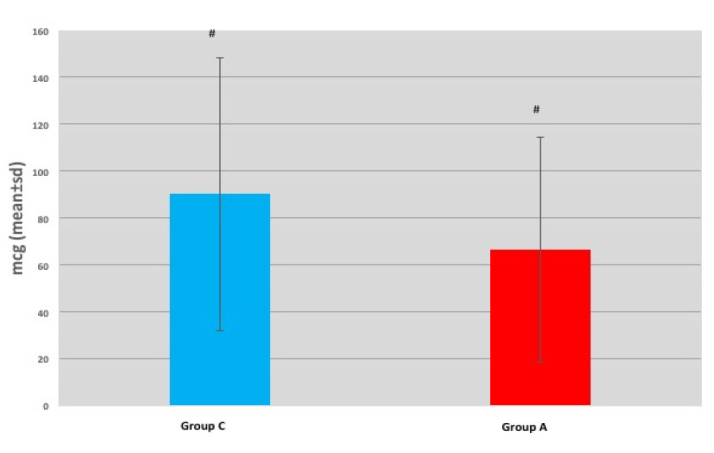
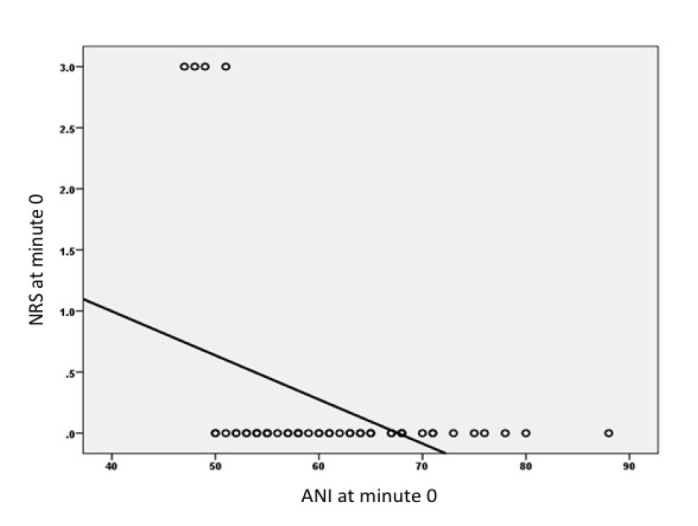
A total remifentanil amount used in Group A was 66.51±47.87 mcg and 90.15±58.17 mcg in Group C (p=0.011); there was no difference in total amounts of ketamine and propofol given. There was a negative correlation between ANI and NRS scores of Group A patients at Minute 0 at the level of 0.402, which was significant statistically (p=0.003).
Opioid consumption was diminished when ANI monitoring was used, and thus the patient safety was improved. Further studies with longer procedure times and with a greater number of patients are required to demonstrate whether there is a difference in side effects and recovery times.
本研究的目的是提高麻醉和镇静下手术过程中的患者舒适度和安全性。镇痛伤害感受指数(ANI)可无创地提供伤害感受与抗伤害感受平衡的信息,可用于客观评估镇痛效果。我们旨在比较使用镇痛管理的传统方法和ANI监测对接受结肠镜检查的患者在使用镇静镇痛时的总阿片类药物消耗量、镇静和镇痛水平的影响。
对计划进行手术镇静的成年患者(n = 102)进行前瞻性分析。在使用丙泊酚和氯胺酮诱导后,开始输注丙泊酚(2 mg·kg⁻¹·h⁻¹)和瑞芬太尼(0.05 mcg·kg⁻¹·min⁻¹)。在A组中,滴定瑞芬太尼输注量以维持ANI值在50至70之间,而在C组中,根据主治麻醉师的意图满足镇痛需求。监测心率、血压、呼吸频率、脉搏血氧饱和度(SpO₂)、脑电双频指数(BIS)、数字评分量表(NRS)和 Ramsay 镇静量表。评估并发症、镇痛药消耗量、手术持续时间、人口统计学信息、NRS和改良Aldrete评分。
A组瑞芬太尼的总用量为66.51±47.87 mcg,C组为90.15±58.17 mcg(p = 0.011);氯胺酮和丙泊酚的总用量无差异。A组患者在第0分钟时ANI与NRS评分之间存在负相关,相关系数为0.402,具有统计学意义(p = 0.003)。
使用ANI监测时阿片类药物消耗量减少,从而提高了患者安全性。需要进行更长手术时间和更多患者的进一步研究,以证明副作用和恢复时间是否存在差异。