From the Department of Medicine, Division of Cardiology (A.A.R., R.H., M.A.G., V.C., D.M., H.R.H., S.N.), and Russell H. Morgan Department of Radiology and Radiological Science (S.L.Z.), Johns Hopkins University, School of Medicine, Baltimore, MD; Department of Radiology, Division of Cardiovascular Imaging, Northwestern University, Feinberg School of Medicine, Chicago, Ill (A.A.R.); Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Harvard Medical School, Boston, Mass (J.E.K.); and Department of Medicine, Division of Cardiology, University of Pennsylvania, Perelman School of Medicine, 3400 Spruce Street, Founders 9, Philadelphia, PA 19104 (S.N.).
Radiology. 2020 May;295(2):307-313. doi: 10.1148/radiol.2020191132. Epub 2020 Mar 3.
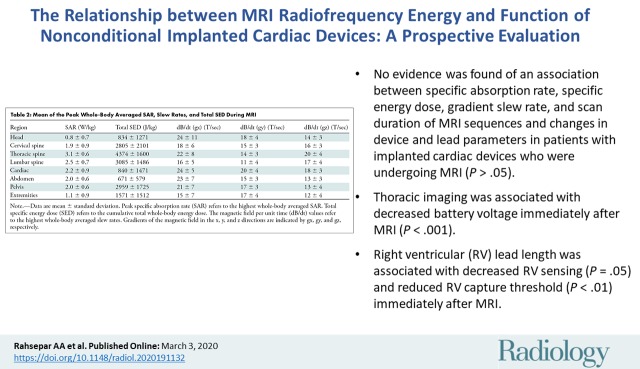
Background The risks associated with MRI in individuals who have implanted cardiac devices are thought to arise from the interaction between the implanted device and static, gradient, and radiofrequency magnetic fields. Purpose To determine the relationship between the peak whole-body averaged specific absorption rate (SAR) and change in magnetic field per unit time (dB/dt), maximum specific energy dose, imaging region, and implanted cardiac device characteristics and their function in patients undergoing MRI. Materials and Methods This prospective observational cohort study was conducted from October 16, 2003, to January 22, 2015 (, NCT01130896). Any individual with an implanted cardiac device who was referred for MRI was included. Clinical MRI protocols without SAR restriction were used. Exclusion criteria were newly implanted leads, abandoned or epicardial leads, and dependence on a pacemaker with an implantable cardioverter defibrillator without asynchronous pacing capability. For each MRI pulse sequence, the calculated whole-body values for SAR, dB/dt, and scan duration were collected. Atrial and ventricular sensing, lead impedance, and capture threshold were evaluated before and immediately after (within 10 minutes) completion of each MRI examination. Generalized estimating equations with Gaussian family, identity link, and an exchangeable working correlation matrix were used for statistical analysis. Results A total of 2028 MRI examinations were performed in 1464 study participants with 2755 device leads (mean age, 67 years ± 15 [standard deviation]; 930 men [64%]). There was no evidence of an association between radiofrequency energy deposition, dB/dt, or scan duration and changes in device parameters. Thoracic MRI was associated with decreased battery voltage immediately after MRI (β = -0.008 V, < .001). Additionally, right ventricular (RV) lead length was associated with decreased RV sensing (β = -0.012 mV, .05) and reduced RV capture threshold (β = -0.002 V, < .01) immediately after MRI. Conclusion There was no evidence of an association between MRI parameters that characterize patient exposure to radiofrequency energy and changes in device and lead parameters immediately after MRI. Nevertheless, device interrogation before and after MRI remains mandatory due to the potential for device reset and changes in lead or generator parameters. © RSNA, 2020 See also the editorial by Shellock in this issue.
背景 人们认为,在植入心脏设备的个体中进行 MRI 会产生风险,这是由于植入设备与静态、梯度和射频磁场之间的相互作用引起的。
目的 确定在接受 MRI 的患者中,峰值全身平均比吸收率 (SAR) 与单位时间内磁场变化 (dB/dt)、最大比能量剂量、成像区域以及植入心脏设备特性及其功能之间的关系。
材料与方法 本前瞻性观察队列研究于 2003 年 10 月 16 日至 2015 年 1 月 22 日进行(NCT01130896)。纳入了任何因 MRI 检查而被转诊的植入心脏设备的个体。使用了没有 SAR 限制的临床 MRI 协议。排除标准为新植入的导联、废弃或心外膜导联以及对没有异步起搏能力的植入式心脏复律除颤器的起搏器的依赖。对于每个 MRI 脉冲序列,收集计算出的全身 SAR、dB/dt 和扫描持续时间值。在每次 MRI 检查前后(10 分钟内)评估心房和心室感知、导联阻抗和捕获阈值。使用具有高斯家族、恒等链接和可交换工作相关矩阵的广义估计方程进行统计分析。
结果 在 1464 名研究参与者的 2755 个设备导联中进行了 2028 次 MRI 检查(平均年龄 67 岁±15[标准差];930 名男性[64%])。没有证据表明射频能量沉积、dB/dt 或扫描持续时间与设备参数的变化之间存在关联。胸部 MRI 与 MRI 后即刻电池电压降低有关(β=-0.008 V,<.001)。此外,右心室 (RV) 导联长度与 RV 感知降低(β=-0.012 mV,<.05)和 RV 捕获阈值降低(β=-0.002 V,<.01)有关。
结论 没有证据表明描述患者暴露于射频能量的 MRI 参数与 MRI 后设备和导联参数的变化之间存在关联。然而,由于设备重置和导联或发生器参数的变化,MRI 前后仍需对设备进行检查。