London School of Hygiene and Tropical Medicine Faculty of Public Health and Policy, London, UK.
Population Health Research Institute, Hamilton Health Sciences and McMaster University, Hamilton, Ontario, Canada.
BMJ Glob Health. 2020 Feb 11;5(2):e002040. doi: 10.1136/bmjgh-2019-002040. eCollection 2020.
Non-communicable diseases (NCDs) are the leading cause of death globally. In 2014, the United Nations committed to reducing premature mortality from NCDs, including by reducing the burden of healthcare costs. Since 2014, the Prospective Urban and Rural Epidemiology (PURE) Study has been collecting health expenditure data from households with NCDs in 18 countries.
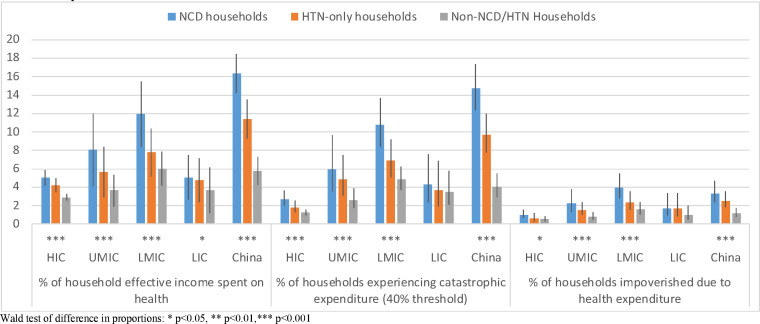
Using data from the PURE Study, we estimated risk of catastrophic health spending and impoverishment among households with at least one person with NCDs (cardiovascular disease, diabetes, kidney disease, cancer and respiratory diseases; n=17 435), with hypertension only (a leading risk factor for NCDs; n=11 831) or with neither (n=22 654) by country income group: high-income countries (Canada and Sweden), upper middle income countries (UMICs: Brazil, Chile, Malaysia, Poland, South Africa and Turkey), lower middle income countries (LMICs: the Philippines, Colombia, India, Iran and the Occupied Palestinian Territory) and low-income countries (LICs: Bangladesh, Pakistan, Zimbabwe and Tanzania) and China.
The prevalence of catastrophic spending and impoverishment is highest among households with NCDs in LMICs and China. After adjusting for covariates that might drive health expenditure, the absolute risk of catastrophic spending is higher in households with NCDs compared with no NCDs in LMICs (risk difference=1.71%; 95% CI 0.75 to 2.67), UMICs (0.82%; 95% CI 0.37 to 1.27) and China (7.52%; 95% CI 5.88 to 9.16). A similar pattern is observed in UMICs and China for impoverishment. A high proportion of those with NCDs in LICs, especially women (38.7% compared with 12.6% in men), reported not taking medication due to costs.
Our findings show that financial protection from healthcare costs for people with NCDs is inadequate, particularly in LMICs and China. While the burden of NCD care may appear greatest in LMICs and China, the burden in LICs may be masked by care foregone due to costs. The high proportion of women reporting foregone care due to cost may in part explain gender inequality in treatment of NCDs.
非传染性疾病(NCDs)是全球死亡的主要原因。2014 年,联合国承诺通过降低医疗保健成本来减少 NCD 导致的过早死亡。自 2014 年以来,前瞻性城乡流行病学(PURE)研究一直在从 18 个国家的 NCD 患者家庭中收集卫生支出数据。
利用 PURE 研究的数据,我们根据国家收入组(高收入国家:加拿大和瑞典;中上收入国家:巴西、智利、马来西亚、波兰、南非和土耳其;中下收入国家:菲律宾、哥伦比亚、印度、伊朗和被占领巴勒斯坦领土;低收入国家:孟加拉国、巴基斯坦、津巴布韦和坦桑尼亚以及中国),分别估算了患有 NCD(心血管疾病、糖尿病、肾病、癌症和呼吸系统疾病;n=17435)、仅有高血压(NCD 的主要危险因素;n=11831)或两者都没有(n=22654)的家庭中灾难性卫生支出和贫困的风险。
中低收入国家和中国 NCD 患者家庭的灾难性支出和贫困发生率最高。在调整了可能导致卫生支出的协变量后,与无 NCD 家庭相比,中低收入国家(风险差异=1.71%;95%CI 0.75 至 2.67)、中上收入国家(0.82%;95%CI 0.37 至 1.27)和中国(7.52%;95%CI 5.88 至 9.16)NCD 患者家庭发生灾难性支出的绝对风险更高。中低收入国家和中国在贫困方面也存在类似的模式。在中低收入国家,特别是女性(38.7%,而男性为 12.6%),由于费用问题,有很大比例的 NCD 患者未服药。
我们的研究结果表明,NCD 患者的医疗保健费用没有得到充分的财务保护,特别是在中低收入国家和中国。虽然 NCD 护理的负担在中低收入国家和中国似乎最大,但由于费用而放弃护理可能掩盖了低收入国家的负担。由于费用而放弃护理的女性比例较高,这在一定程度上解释了 NCD 治疗中的性别不平等。