Lichtenegger Felix S, Schnorfeil Frauke M, Rothe Maurine, Deiser Katrin, Altmann Torben, Bücklein Veit L, Köhnke Thomas, Augsberger Christian, Konstandin Nikola P, Spiekermann Karsten, Moosmann Andreas, Boehm Stephan, Boxberg Melanie, Heemskerk Mirjam Hm, Goerlich Dennis, Wittmann Georg, Wagner Beate, Hiddemann Wolfgang, Schendel Dolores J, Kvalheim Gunnar, Bigalke Iris, Subklewe Marion
Department of Medicine III University Hospital, LMU Munich Munich Germany.
Laboratory for Translational Cancer Immunology Gene Center LMU Munich Munich Germany.
Clin Transl Immunology. 2020 Mar 3;9(3):e1117. doi: 10.1002/cti2.1117. eCollection 2020.
Innovative post-remission therapies are needed to eliminate residual AML cells. DC vaccination is a promising strategy to induce anti-leukaemic immune responses.
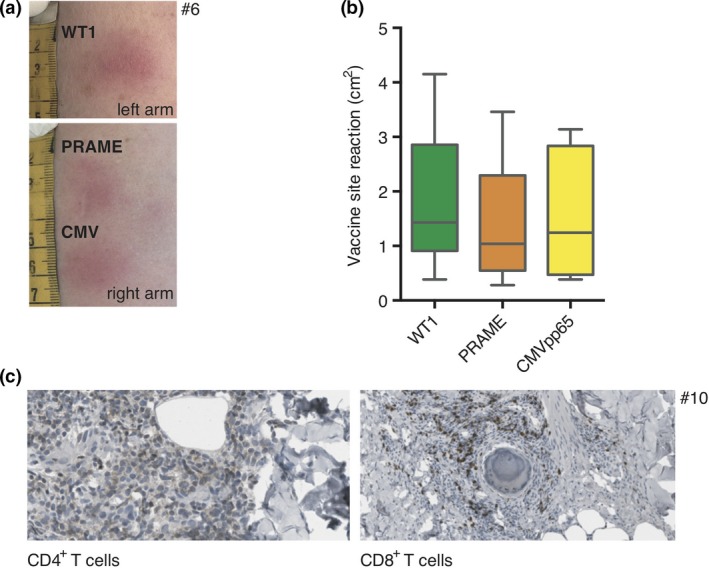
We conducted a first-in-human phase I study using TLR7/8-matured DCs transfected with RNA encoding the two AML-associated antigens WT1 and PRAME as well as CMVpp65. AML patients in CR at high risk of relapse were vaccinated 10× over 26 weeks.
Despite heavy pretreatment, DCs of sufficient number and quality were generated from a single leukapheresis in 11/12 cases, and 10 patients were vaccinated. Administration was safe and resulted in local inflammatory responses with dense T-cell infiltration. In peripheral blood, increased antigen-specific CD8 T cells were seen for WT1 (2/10), PRAME (4/10) and CMVpp65 (9/10). For CMVpp65, increased CD4 T cells were detected in 4/7 patients, and an antibody response was induced in 3/7 initially seronegative patients. Median OS was not reached after 1057 days; median RFS was 1084 days. A positive correlation was observed between clinical benefit and younger age as well as mounting of antigen-specific immune responses.
Administration of TLR7/8-matured DCs to AML patients in CR at high risk of relapse was feasible and safe and resulted in induction of antigen-specific immune responses. Clinical benefit appeared to occur more likely in patients <65 and in patients mounting an immune response. Our observations need to be validated in a larger patient cohort. We hypothesise that TLR7/8 DC vaccination strategies should be combined with hypomethylating agents or checkpoint inhibition to augment immune responses.
The study was registered at https://clinicaltrials.gov on 17 October 2012 (NCT01734304) and at https://www.clinicaltrialsregister.eu (EudraCT-Number 2010-022446-24) on 10 October 2013.
需要创新的缓解后疗法来清除残留的急性髓系白血病(AML)细胞。树突状细胞(DC)疫苗接种是诱导抗白血病免疫反应的一种有前景的策略。
我们开展了一项首次人体I期研究,使用经转染编码两种AML相关抗原WT1和PRAME以及巨细胞病毒(CMV)pp65的RNA而成熟的TLR7/8 DC。处于缓解期且复发风险高的AML患者在26周内接种10次疫苗。
尽管进行了大量预处理,但12例中有11例通过单次白细胞分离术产生了数量充足且质量合格的DC,10例患者接种了疫苗。给药安全,导致局部炎症反应及密集的T细胞浸润。在外周血中,WT1(2/10)、PRAME(4/10)和CMV pp65(9/10)的抗原特异性CD8 T细胞增加。对于CMV pp65,4/7的患者检测到CD4 T细胞增加,3/7最初血清学阴性的患者诱导出抗体反应。1057天后未达到中位总生存期(OS);中位无复发生存期(RFS)为1084天。观察到临床获益与年轻以及抗原特异性免疫反应增强之间存在正相关。
对处于缓解期且复发风险高的AML患者给予TLR7/8成熟的DC是可行且安全的,并能诱导抗原特异性免疫反应。临床获益似乎在<65岁的患者以及产生免疫反应的患者中更易出现。我们的观察结果需要在更大的患者队列中进行验证。我们假设TLR7/8 DC疫苗接种策略应与去甲基化药物或检查点抑制联合使用以增强免疫反应。
该研究于2012年10月17日在https://clinicaltrials.gov注册(NCT01734304),并于2013年10月10日在https://www.clinicaltrialsregister.eu注册(欧盟临床试验编号2010 - 022446 - 24)。