Parker Robert K, Mwachiro Elizabeth B, Mwachiro Michael M, Pletcher Jocelyn, Parker Andrea S, Many Heath R
Department of Surgery, Tenwek Hospital, Bomet, Kenya.
Department of Surgery, Alpert Medical School of Brown University, Providence, RI.
Crit Care Explor. 2019 Dec 10;1(12):e0067. doi: 10.1097/CCE.0000000000000067. eCollection 2019 Dec.
Critical care is expanding in low- and middle-income countries. Yet, due to factors such as missing data and different disease patterns, predictive scores often fail to adequately predict the high rates of mortality observed.
We evaluated multiple prognostic models for the outcome of mortality in critically ill, mechanically ventilated patients in rural Kenya and examined factors contributing to mortality in our setting.
A prospective cohort study was conducted on mechanically ventilated patients in rural Kenya. Consecutive patients 16 years old and older initiated on mechanical ventilation between January 1, 2016, and April 30, 2017, at Tenwek Hospital were included. Demographic data, clinical characteristics, and patient outcomes were collected during routine clinical care.
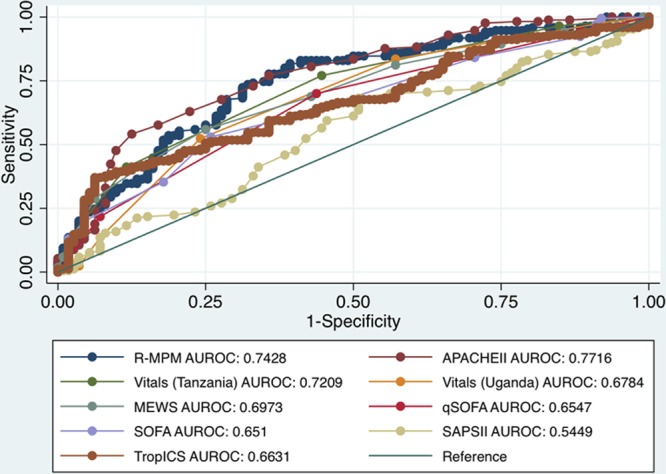
We assessed the discrimination and calibration of multiple previously-described models for mortality: Acute Physiology and Chronic Health Evaluation II, Sequential Organ Failure Assessment, quick Sequential Organ Failure Assessment, Simplified Acute Physiology Score II, Modified Early Warning Score, Tropical Intensive Care Score, Rwanda-Mortality Predictive Model, Vitals score (validated in Tanzania), and Vitals score for sepsis (validated in Uganda). Factors most associated with mortality were analyzed in our cohort utilizing stepwise regression.
Among the final cohort of 300 patients, the overall mortality rate was 60.7%, the average age was 39.9 years, 65% were male, and 33% were seen at an outside facility prior to admission to the critical care unit. Missing variables occurred in patients for numerous models but were complete in most adapted to resource-limited settings. Models displayed moderate prediction of mortality and variable discrimination area under the receiver operating characteristic curves (and Hosmer-Lemeshow chi-square statistic) of 0.77 (22.4) for Acute Physiology and Chronic Health Evaluation II, 0.70 (3.4) for Modified Early Warning Score, 0.65 (0.16) for quick Sequential Organ Failure Assessment, 0.55 (18.4) for Simplified Acute Physiology Score II and 0.74 (9.2) for Rwanda-Mortality Predictive Model, 0.72 (0.12) for Vitals Tanzania, 0.68 (14.7) for Vitals Uganda, and 0.65 (13.9) for Tropical Intensive Care Score. Variables associated with increased mortality in our population were hypotension, infection, traumatic brain injury, and hematocrit.
Overall, survival for critically ill patients in rural Kenya was poor, but predictable with contributing factors. Models designed for resource-constrained settings had favorable discrimination and better calibration for mortality prediction than high-resource models in our population of mechanically ventilated, critically ill patients in rural Kenya.
重症监护在低收入和中等收入国家正在扩大。然而,由于数据缺失和疾病模式不同等因素,预测评分往往无法充分预测所观察到的高死亡率。
我们评估了多种用于肯尼亚农村地区重症机械通气患者死亡率结局的预后模型,并研究了导致我们研究环境中死亡率的因素。
设计、设置和参与者:对肯尼亚农村地区的机械通气患者进行了一项前瞻性队列研究。纳入了2016年1月1日至2017年4月30日在滕韦克医院开始接受机械通气的16岁及以上连续患者。在常规临床护理期间收集了人口统计学数据、临床特征和患者结局。
我们评估了多种先前描述的死亡率模型的区分度和校准度:急性生理与慢性健康状况评价II(APACHE II)、序贯器官衰竭评估(SOFA)、快速序贯器官衰竭评估(qSOFA)、简化急性生理评分II(SAPS II)、改良早期预警评分(MEWS)、热带重症监护评分(TICS)、卢旺达死亡率预测模型(RMPM)、生命体征评分(在坦桑尼亚验证)和脓毒症生命体征评分(在乌干达验证)。利用逐步回归分析了我们队列中与死亡率最相关的因素。
在最终的300例患者队列中,总体死亡率为60.7%,平均年龄为39.9岁,65%为男性,33%在入住重症监护病房之前曾在外部机构就诊。许多模型的患者存在变量缺失,但大多数适用于资源有限环境的模型变量完整。模型对死亡率的预测表现中等,在接受者操作特征曲线下的区分度区域(以及Hosmer-Lemeshow卡方统计量)有所不同:APACHE II为0.77(22.4),MEWS为0.70(3.4),qSOFA为0.65(0.16),SAPS II为0.55(18.4),RMPM为0.74(9.2),坦桑尼亚生命体征评分为0.72(0.12),乌干达生命体征评分为0.68(14.7),TICS为0.65(13.9)。与我们研究人群中死亡率增加相关的变量是低血压、感染、创伤性脑损伤和血细胞比容。
总体而言,肯尼亚农村地区重症患者的生存率较低,但可通过相关因素进行预测。在我们肯尼亚农村地区机械通气的重症患者人群中,为资源受限环境设计的模型在死亡率预测方面比高资源模型具有更好的区分度和校准度。