Toivonen Laura, Schuez-Havupalo Linnea, Karppinen Sinikka, Waris Matti, Hoffman Kristi L, Camargo Carlos A, Hasegawa Kohei, Peltola Ville
Department of Emergency Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA.
Department of Pediatrics and Adolescent Medicine, Turku University Hospital and University of Turku, Turku, Finland.
Clin Infect Dis. 2021 May 4;72(9):1546-1554. doi: 10.1093/cid/ciaa262.
Early-life exposures to antibiotics may increase the risk of developing childhood asthma. However, little is known about the mechanisms linking antibiotic exposures to asthma. We hypothesized that changes in the nasal airway microbiota serve as a causal mediator in the antibiotics-asthma link.
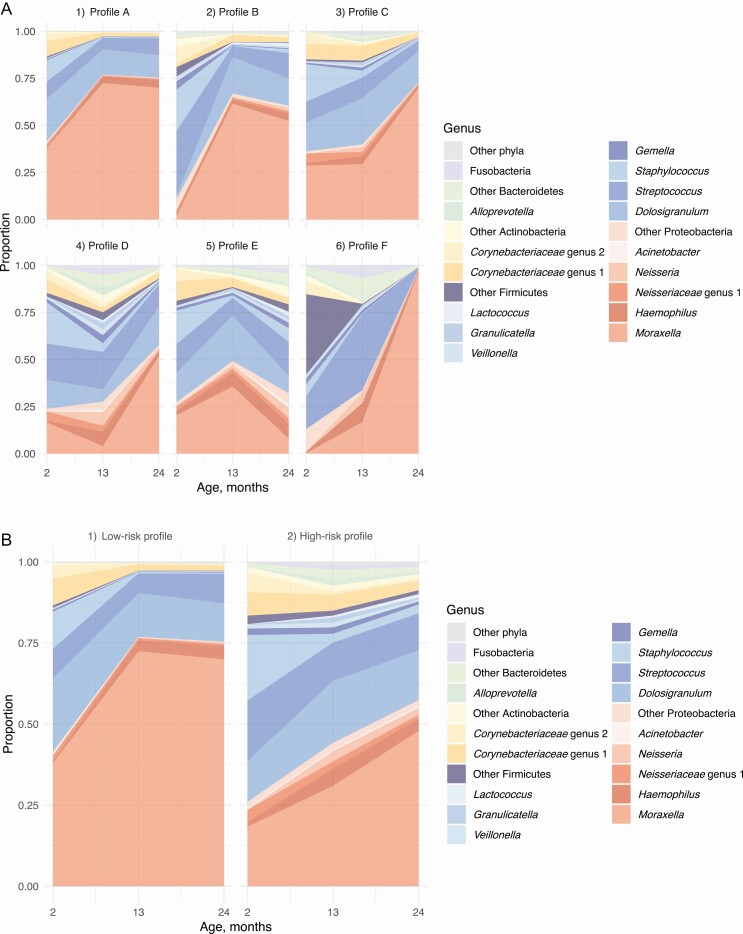
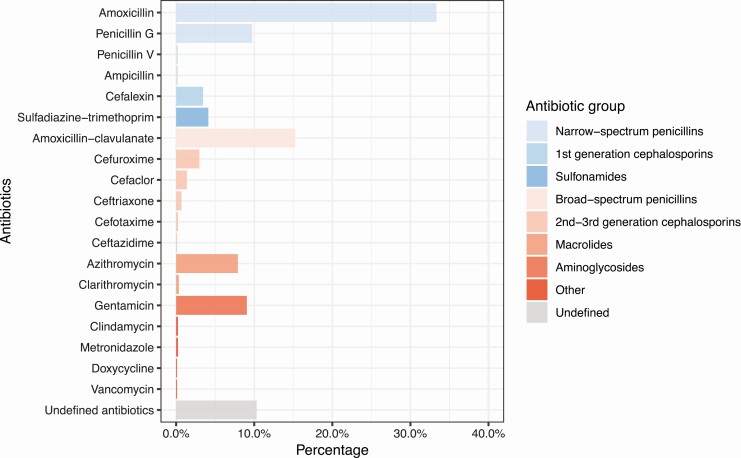
In a population-based birth-cohort study in Finland, we identified longitudinal nasal microbiota profiles during age 2-24 months using 16S rRNA gene sequencing and an unsupervised machine learning approach. We performed a causal mediation analysis to estimate the natural direct effect of systemic antibiotic treatments during age 0-11 months on risks of developing physician-diagnosed asthma by age 7 years and the natural indirect (causal mediation) effect through longitudinal changes in nasal microbiota.
In our birth cohort of 697 children, 8.0% later developed asthma. Exposure to ≥2 antibiotic treatments during age 0-11 months was associated with a 4.0% increase in the absolute risk of developing asthma (absolute increase, 95% CI, .9-7.2%; P = .006). The unsupervised clustering approach identified 6 longitudinal nasal microbiota profiles. Infants with a larger number of antibiotic treatments had a higher risk of having a profile with early Moraxella sparsity (per each antibiotic treatment, adjusted RRR, 1.38; 95% CI, 1.15-1.66; P < .001). This effect of antibiotics on asthma was partly mediated by longitudinal changes in the nasal microbiota (natural indirect effect, P = .008), accounting for 16% of the total effect.
Early exposures to antibiotics were associated with increased risk of asthma; the effect was mediated, in part, by longitudinal changes in the nasal airway microbiota.
儿童早期接触抗生素可能会增加患儿童哮喘的风险。然而,关于抗生素接触与哮喘之间的联系机制知之甚少。我们推测鼻气道微生物群的变化是抗生素与哮喘联系的因果中介。
在芬兰一项基于人群的出生队列研究中,我们使用16S rRNA基因测序和无监督机器学习方法确定了2至24个月龄期间的纵向鼻微生物群谱。我们进行了因果中介分析,以估计0至11个月龄期间全身抗生素治疗对7岁时医生诊断哮喘风险的自然直接效应,以及通过鼻微生物群的纵向变化产生的自然间接(因果中介)效应。
在我们697名儿童的出生队列中,8.0%的儿童后来患了哮喘。0至11个月龄期间接触≥2次抗生素治疗与患哮喘的绝对风险增加4.0%相关(绝对增加,95%CI,0.9-7.2%;P = 0.006)。无监督聚类方法确定了6种纵向鼻微生物群谱。接受更多抗生素治疗的婴儿出现早期莫拉菌稀疏型的风险更高(每次抗生素治疗,调整后的相对风险率,1.38;95%CI,1.15-1.66;P < 0.001)。抗生素对哮喘的这种影响部分是由鼻微生物群的纵向变化介导的(自然间接效应,P = 0.008),占总效应的16%。
早期接触抗生素与哮喘风险增加有关;这种影响部分是由鼻气道微生物群的纵向变化介导的。