Barsosio Hellen C, Gitonga John N, Karanja Henry K, Nyamwaya Doris K, Omuoyo Donwilliams O, Kamau Everlyn, Hamaluba Mainga M, Nyiro Joyce U, Kitsao Barnes S, Nyaguara Amek, Mwakio Stella, Newton Charles R, Sang Rosemary, Wright Daniel, Sanders Eduard J, Seale Anna C, Agoti Charles N, Berkley James A, Bejon Philip, Warimwe George M
KEMRI-Wellcome Trust Research Programme, Kilifi, Kenya.
Liverpool School of Tropical Medicine, Liverpool, UK.
Wellcome Open Res. 2019 Nov 15;4:179. doi: 10.12688/wellcomeopenres.15568.1. eCollection 2019.
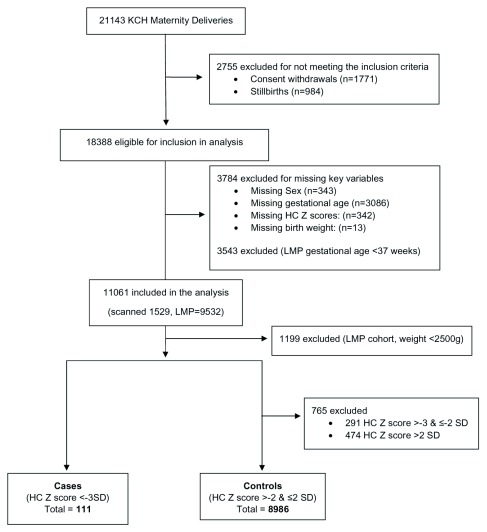
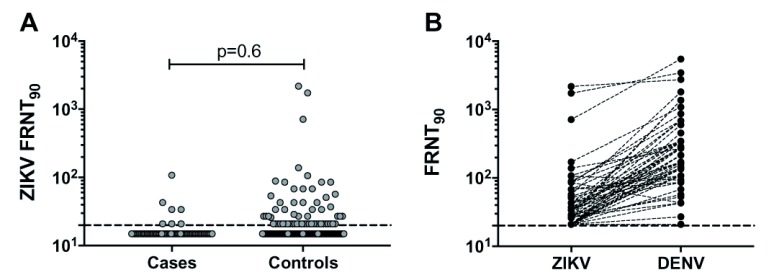
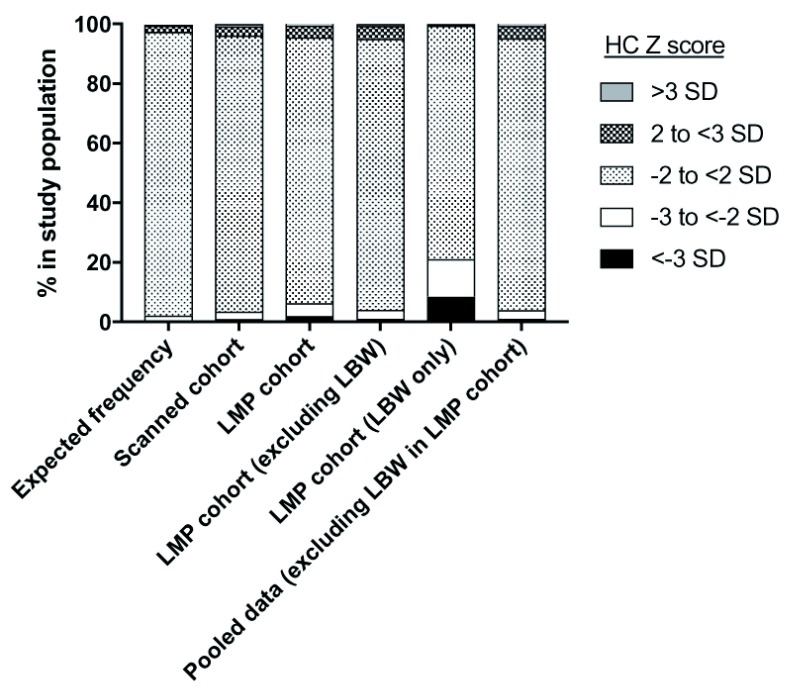
Zika virus (ZIKV) was first discovered in East Africa in 1947. ZIKV has caused microcephaly in the Americas, but it is not known whether ZIKV is a cause of microcephaly in East Africa. We used surveillance data from 11,061 live births at Kilifi County Hospital in coastal Kenya between January 2012 and October 2016 to identify microcephaly cases and conducted a nested case-control study to determine risk factors for microcephaly. Gestational age at birth was estimated based on antenatal ultrasound scanning ('Scanned cohort') or last menstrual period ('LMP cohort', including births ≥37 weeks' gestation only). Controls were newborns with head circumference Z scores between >-2 and ≤2 SD that were compared to microcephaly cases in relation to ZIKV exposure and other maternal and newborn factors. Of the 11,061 newborns, 214 (1.9%, 95%CI 1.69, 2.21) had microcephaly. Microcephaly prevalence was 1.0% (95%CI 0.64, 1.70, n=1529) and 2.1% (95%CI 1.81, 2.38, n=9532) in the scanned and LMP cohorts, respectively. After excluding babies <2500 g (n=1199) in the LMP cohort the prevalence was 1.1% (95%CI 0.93, 1.39). Microcephaly showed an association with being born small for gestational age (p<0.001) but not with ZIKV neutralising antibodies (p=0.6) or anti-ZIKV NS1 IgM response (p=0.9). No samples had a ZIKV neutralising antibody titre that was at least fourfold higher than the corresponding dengue virus (DENV) titre. No ZIKV or other flavivirus RNA was detected in cord blood from cases or controls. Microcephaly was prevalent in coastal Kenya, but does not appear to be related to ZIKV exposure; the ZIKV response observed in our study population was largely due to cross-reactive responses to DENV or other related flaviviruses. Further research into potential causes and the clinical consequences of microcephaly in this population is urgently needed.
寨卡病毒(ZIKV)于1947年在东非首次被发现。寨卡病毒在美洲导致了小头畸形,但在东非它是否是小头畸形的病因尚不清楚。我们利用了2012年1月至2016年10月间肯尼亚沿海基利菲县医院11061例活产的监测数据来确定小头畸形病例,并进行了一项巢式病例对照研究以确定小头畸形的危险因素。根据产前超声扫描(“超声队列”)或末次月经日期(“LMP队列”,仅包括孕周≥37周的分娩)来估计出生时的孕周。对照为头围Z评分在>-2至≤2标准差之间的新生儿,将其与小头畸形病例在寨卡病毒暴露及其他母婴因素方面进行比较。在这11061例新生儿中,214例(1.9%,95%置信区间1.69, 2.21)患有小头畸形。小头畸形患病率在超声队列中为1.0%(95%置信区间0.64, 1.70,n = 1529),在LMP队列中为2.1%(95%置信区间1.81, 2.38,n = 9532)。在LMP队列中排除体重<2500g的婴儿(n = 1199)后,患病率为1.1%(95%置信区间0.93, 1.39)。小头畸形与小于胎龄儿出生有关(p<0.001),但与寨卡病毒中和抗体(p = 0.6)或抗寨卡病毒NS1 IgM反应(p = 0.9)无关。没有样本的寨卡病毒中和抗体滴度比相应的登革病毒(DENV)滴度至少高四倍。在病例组或对照组的脐带血中未检测到寨卡病毒或其他黄病毒RNA。小头畸形在肯尼亚沿海地区很普遍,但似乎与寨卡病毒暴露无关;我们研究人群中观察到的寨卡病毒反应很大程度上是由于对登革病毒或其他相关黄病毒的交叉反应。迫切需要对该人群中小头畸形的潜在病因和临床后果进行进一步研究。