Purcell Laura N, Tignanelli Christopher J, Maine Rebecca, Charles Anthony
From the *Department of Surgery, University of North Carolina, Chapel Hill, North Carolina.
†Division of Acute Care Surgery, Department of Surgery, University of Minnesota, Minneapolis, Minnesota.
Am Surg. 2020 Mar 1;86(3):237-244.
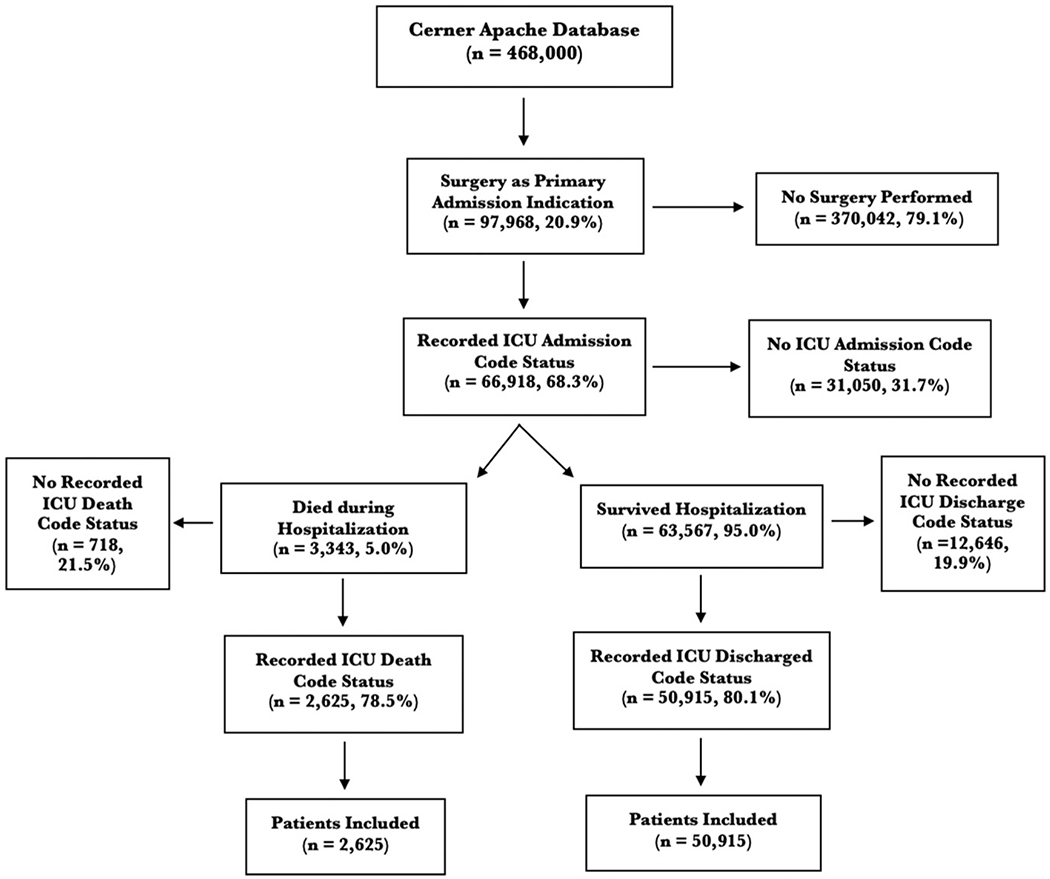
Racial and gender disparities in end-of-life decision-making practices have not been well described in surgical patients. We performed an eight-year retrospective analysis of surgical patients within the Cerner Acute Physiology and Chronic Health Evaluation Outcomes database. ICU patients with documented admission code status, and death or ICU discharge code status, respectively, were included. Logistic regression analysis was performed to assess change in code status. Of 468,000 ICU patients, 97,968 (20.9%) were surgical, 63,567 (95%) survived, and 3,343 (5%) died during their hospitalization. Of those, 50,915 (80.1%) and 2,625 (78.5%) had complete code status data on admission and discharge or death, respectively. Women were less likely than men to remain full code at ICU discharge and death (n = 20,940, 95.6% and n = 141, 11.9% n = 29,320, 97.4% and n = 233, 16.3%, < 0.001). Compared with whites, blacks and other minorities had a 0.46 odds (95% confidence interval [CI]: 0.33-0.64, < 0.001) and 0.54 odds (95% CI: 0.34-0.85, = 0.01) of changing from full code status before death, respectively. Before ICU discharge, blacks and other minorities had a 0.56 odds of changing from full code status when compared with whites (95% CI: 0.40-0.79, < 0.001 95% CI: 0.36-0.87, = 0.01, respectively). Women were more likely to be discharged or die after a change in code status from full code (odds ratio 1.27, 95% CI: 1.06-1.07, < 0.001; odds ratio 1.39, 95% CI: 1.09-1.79, = 0.009). Men and minorities are more likely to be discharged from the ICU or die with a full code status designation.
临终决策实践中的种族和性别差异在外科手术患者中尚未得到充分描述。我们对Cerner急性生理学和慢性健康评估结果数据库中的外科手术患者进行了为期八年的回顾性分析。纳入了分别有记录在案的入院代码状态以及死亡或重症监护病房(ICU)出院代码状态的ICU患者。进行逻辑回归分析以评估代码状态的变化。在468,000名ICU患者中,97,968名(20.9%)为外科手术患者,63,567名(95%)存活,3,343名(5%)在住院期间死亡。其中,50,915名(80.1%)和2,625名(78.5%)分别在入院时以及出院或死亡时有完整的代码状态数据。在ICU出院和死亡时,女性保持完全代码状态的可能性低于男性(n = 20,940,95.6%;n = 141,11.9%;n = 29,320,97.4%;n = 233,16.3%,P < 0.001)。与白人相比,黑人和其他少数族裔在死亡前从完全代码状态转变的几率分别为0.46(95%置信区间[CI]:0.33 - 0.64,P < 0.001)和0.54(95% CI:0.34 - 0.85,P = 0.01)。在ICU出院前,与白人相比,黑人和其他少数族裔从完全代码状态转变的几率分别为0.56(95% CI:0.40 - 0.79,P < 0.001)和0.56(95% CI:0.36 - 0.87,P = 0.01)。女性在代码状态从完全代码转变后更有可能出院或死亡(优势比1.27,95% CI:1.06 - 1.07,P < 0.001;优势比1.39,95% CI:1.09 - 1.79,P = 0.009)。男性和少数族裔更有可能以完全代码状态从ICU出院或死亡。