Department of Epidemiology and Biostatistics, Western University, 1151 Richmond St., London, ON, N6A 5C1, Canada.
Department of Family Medicine, Western University, 1151 Richmond St., London, ON, N6A 5C1, Canada.
BMC Pregnancy Childbirth. 2020 Mar 31;20(1):194. doi: 10.1186/s12884-020-02879-y.
While maternal mortality has declined worldwide in the past 25 years, this is not the case for Cameroon. Since there is a predominantly young population in this country, high maternal mortality ratios may persist. Maternal mortality ratios vary within countries, yet it is unknown if the North and South, the most distinct parts of Cameroon, differ in terms of ratios and determinants of maternal mortality.
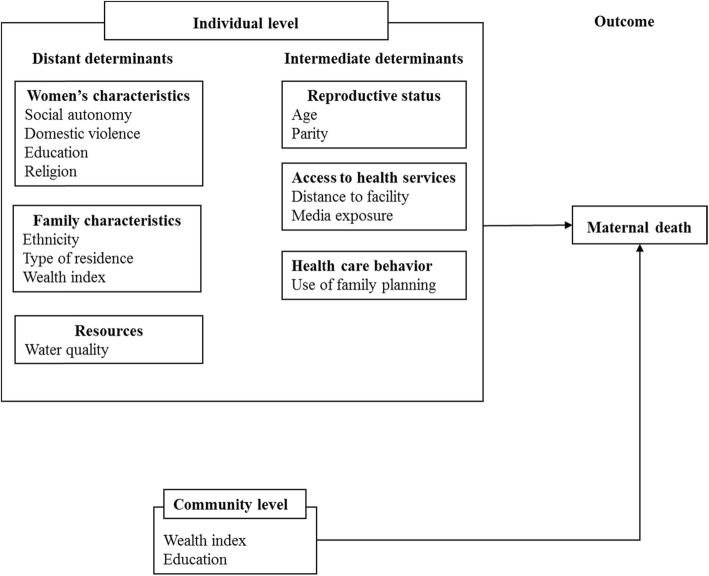
This study explored ratios and determinants of maternal mortality in women of childbearing age (15-49 years) and assessed differences between the North and South. We used the Cameroon Demographic and Health Surveys (2004 and 2011) to extract a sample of 18,665 living or deceased women who had given birth. Multivariable logistic regression was used to explore the relationship between maternal mortality and sociocultural, economic and healthcare factors.
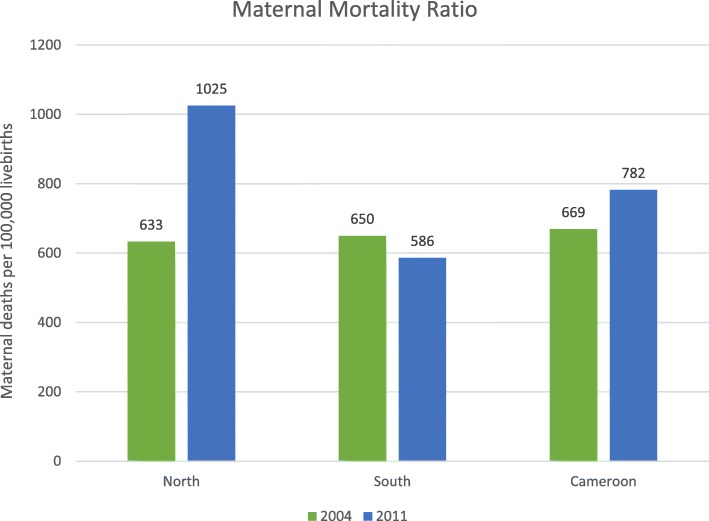
Maternal mortality ratios were different for the two regions and increased in the North in 2011 compared to 2004. In the North, any level of education and being Muslim were protective against maternal mortality. Meanwhile, the odds of maternal mortality decreased with increasing age, and having secondary or higher education in the South. Domestic violence and ethnicity were associated with maternal death in the South. Increasing parity was protective of maternal death in both the North and South.
Maternal mortality ratios and determinants varied between women of childbearing age in the North and South of Cameroon. These reinforce recommendations for region specific strategies that will improve health communication, community education programs, curb domestic violence and train more community health workers to connect pregnant women with the health system. Programs to reduce maternal death among women with low parity and little or no education should be national priority.
尽管在过去的 25 年中,全球范围内的产妇死亡率有所下降,但喀麦隆并非如此。由于该国人口主要以年轻人为主,因此高产妇死亡率可能会持续存在。产妇死亡率在各国之间存在差异,但尚不清楚喀麦隆最具特色的北部和南部在产妇死亡率的比率和决定因素方面是否存在差异。
本研究探讨了育龄妇女(15-49 岁)的产妇死亡率比率和决定因素,并评估了北部和南部之间的差异。我们使用喀麦隆人口与健康调查(2004 年和 2011 年)提取了一个由 18665 名活产或死亡的生育妇女组成的样本。多变量逻辑回归用于探讨产妇死亡率与社会文化、经济和医疗保健因素之间的关系。
两个地区的产妇死亡率比率不同,2011 年北部的比率较 2004 年有所增加。在北部,任何程度的教育和穆斯林身份都对产妇死亡率具有保护作用。而在南部,产妇死亡率的几率随着年龄的增长而降低,并且在南部接受中等或高等教育也会降低产妇死亡率。在南部,家庭暴力和族裔与产妇死亡有关。在北部和南部,增加生育次数都可以保护产妇免受死亡。
喀麦隆北部和南部育龄妇女的产妇死亡率比率和决定因素有所不同。这些因素强化了针对特定地区的策略的建议,这些策略将改善健康传播、社区教育计划、遏制家庭暴力和培训更多的社区卫生工作者,以将孕妇与卫生系统联系起来。减少低生育次数和受教育程度低或未受教育的妇女的产妇死亡率应成为国家优先事项。