Section of Cardiology, Department of Medicine (B.S., J.D.L., N.R.S.), VA New York Harbor Health Care System.
Division of Cardiology, Department of Medicine (B.S., J.D.L., N.R.S., F.F., N.R., N.M.K., S.D.K.), New York University School of Medicine.
Circ Cardiovasc Interv. 2020 Apr;13(4):e008717. doi: 10.1161/CIRCINTERVENTIONS.119.008717. Epub 2020 Apr 16.
Vascular injury and inflammation during percutaneous coronary intervention (PCI) are associated with increased risk of post-PCI adverse outcomes. Colchicine decreases neutrophil recruitment to sites of vascular injury. The anti-inflammatory effects of acute colchicine administration before PCI on subsequent myocardial injury are unknown.
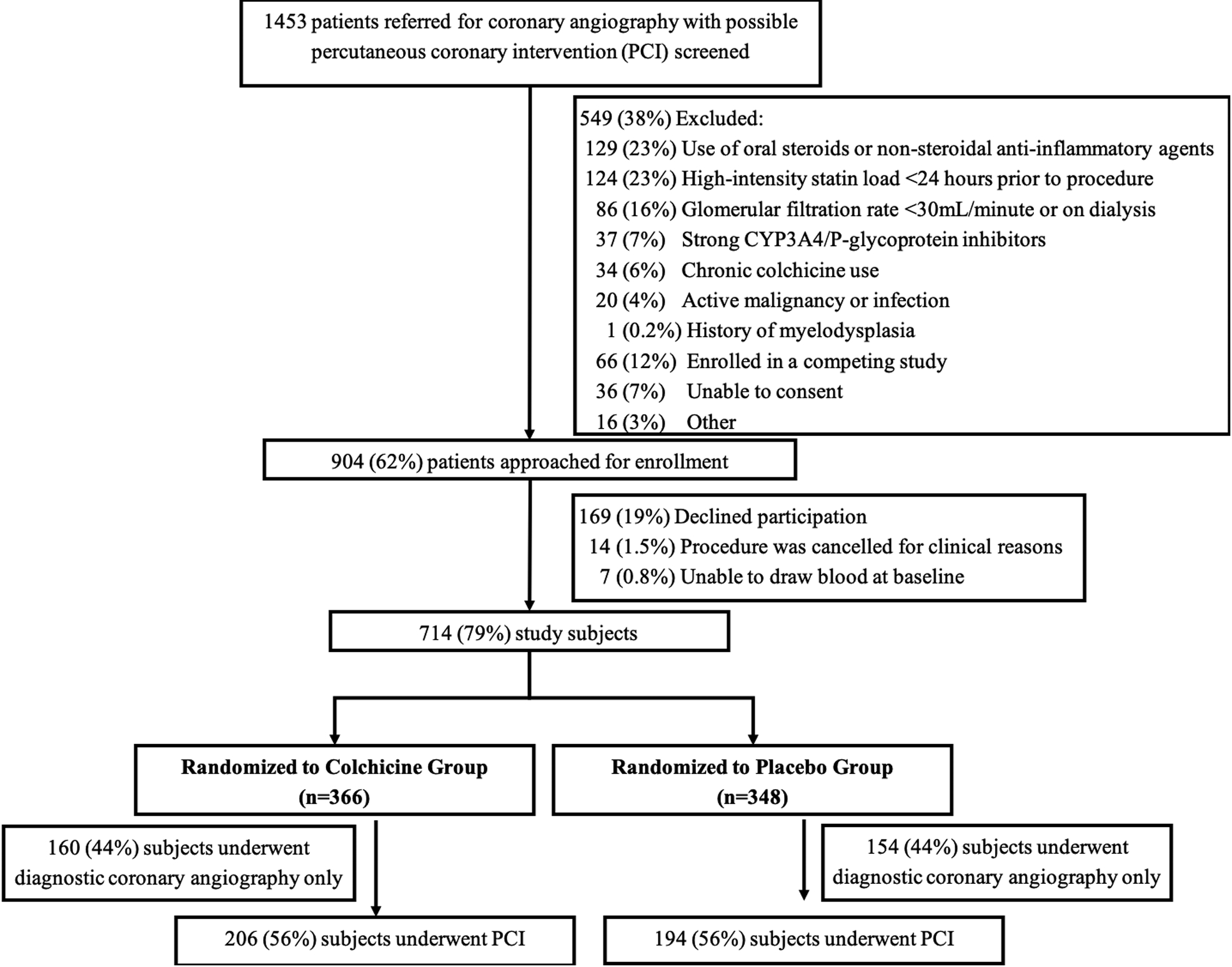
In a prospective, single-site trial, subjects referred for possible PCI (n=714) were randomized to acute preprocedural oral administration of colchicine 1.8 mg or placebo.
Among the 400 subjects who underwent PCI, the primary outcome of PCI-related myocardial injury did not differ between colchicine (n=206) and placebo (n=194) groups (57.3% versus 64.2%, =0.19). The composite outcome of death, nonfatal myocardial infarction, and target vessel revascularization at 30 days (11.7% versus 12.9%, =0.82), and the outcome of PCI-related myocardial infarction defined by the Society for Cardiovascular Angiography and Interventions (2.9% versus 4.7%, =0.49) did not differ between colchicine and placebo groups. Among 280 PCI subjects in a nested inflammatory biomarker substudy, the primary biomarker end point, change in interleukin-6 concentrations did not differ between groups 1-hour post-PCI but increased less 24 hours post-PCI in the colchicine (n=141) versus placebo group (n=139; 76% [-6 to 898] versus 338% [27 to 1264], =0.02). High-sensitivity C-reactive protein concentration also increased less after 24 hours in the colchicine versus placebo groups (11% [-14 to 80] versus 66% [1 to 172], =0.001).
Acute preprocedural administration of colchicine attenuated the increase in interleukin-6 and high-sensitivity C-reactive protein concentrations after PCI when compared with placebo but did not lower the risk of PCI-related myocardial injury. Registration: URL: https://www.clinicaltrials.gov; Unique Identifiers: NCT02594111, NCT01709981.
经皮冠状动脉介入治疗(PCI)过程中的血管损伤和炎症与 PCI 后不良结局的风险增加有关。秋水仙碱可减少中性粒细胞向血管损伤部位的募集。急性 PCI 前秋水仙碱给药对随后心肌损伤的抗炎作用尚不清楚。
在一项前瞻性、单中心试验中,将 714 名拟行 PCI 的患者随机分为急性 PCI 前口服秋水仙碱 1.8mg 或安慰剂组。
在 400 名接受 PCI 的患者中,秋水仙碱组(n=206)和安慰剂组(n=194)的 PCI 相关心肌损伤的主要结局无差异(57.3%比 64.2%,=0.19)。30 天的死亡、非致死性心肌梗死和靶血管血运重建的复合终点(11.7%比 12.9%,=0.82)以及心血管造影和介入学会定义的 PCI 相关心肌梗死的结局(2.9%比 4.7%,=0.49)在秋水仙碱组和安慰剂组之间无差异。在一项嵌套炎症生物标志物亚研究的 280 名 PCI 患者中,1 小时时两组的主要生物标志物终点,白细胞介素-6 浓度无差异,但秋水仙碱组(n=141)24 小时时增加较少(76%[-6 至 898]比安慰剂组 338%[27 至 1264],=0.02)。24 小时时,秋水仙碱组的高敏 C 反应蛋白浓度升高也较安慰剂组少(11%[-14 至 80]比安慰剂组 66%[1 至 172],=0.001)。
与安慰剂相比,急性 PCI 前应用秋水仙碱可减轻 PCI 后白细胞介素-6 和高敏 C 反应蛋白浓度的升高,但不能降低 PCI 相关心肌损伤的风险。注册:网址:https://www.clinicaltrials.gov;唯一标识符:NCT02594111,NCT01709981。