Sullivan Emma, Kershaw Jim, Blackburn Stuart, Choi Jeannie, Curtis Jeffrey R, Boklage Susan
Adelphi Real World, Macclesfield, UK.
Sanofi, Bridgewater, NJ, USA.
Rheumatol Ther. 2020 Jun;7(2):383-400. doi: 10.1007/s40744-020-00203-w. Epub 2020 Apr 21.
Some patients with rheumatoid arthritis (RA) using tumor necrosis factor inhibitors (TNFi) experience inefficacy or lack of tolerability and hence switch to another TNFi (cycling) or to a therapy with another mode of action (switching). This study examined patient characteristics, prescribing patterns and treatment practice for RA in the United States.
Data were from the Adelphi Disease Specific Programme (Q2-Q3 2016). Rheumatologists completed a survey and patient record forms for adult patients with RA who had received ≥ 1 targeted therapy. Patients were grouped by class of first-used targeted therapy, and monotherapy vs. combination therapy. TNFi patients who received ≥ 1 targeted therapy were classified as cyclers or switchers. Univariate analyses compared patient characteristics and physician factors across the analysis groups.
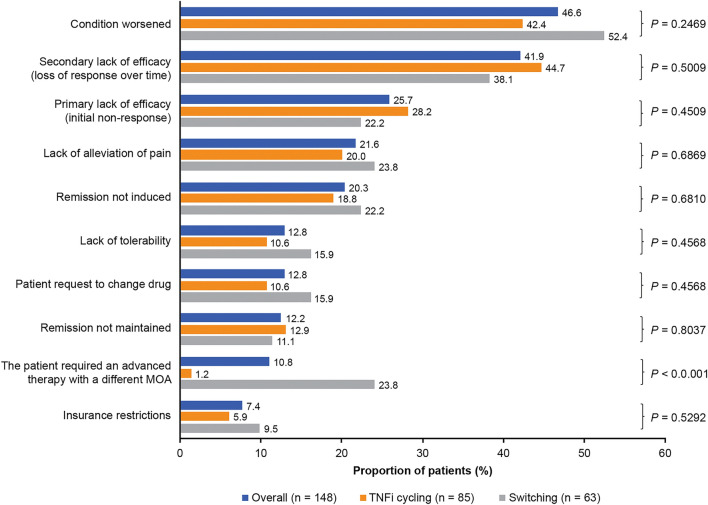
Overall, 631 patients received ≥ 1 targeted therapy; 535 were prescribed a TNFi as first targeted therapy, 53 a nonTNFi biologic disease-modifying antirheumatic drug (bDMARD), and 43 tofacitinib. Of 577 patients with known conventional synthetic (cs) DMARD status, 18.7% were prescribed monotherapy and 81.3% combination therapy. Combination therapy patients received significantly more concomitant medications prior to initiation of first targeted therapy than monotherapy patients (P < 0.05). The top reason for physicians to prescribe first use targeted therapy was strong overall efficacy (79.9%). Of 163 patients who progressed to second targeted therapy, 60.7% were cyclers. A lower proportion of cyclers persisted on their first use targeted therapy versus switchers (P = 0.03). The main reason physicians gave for switching patients at this stage was worsening condition (46.6%).
Most patients were prescribed a TNFi as their first targeted therapy; over half then cycled to another TNFi. This suggests other factors may influence second use targeted treatment choice and highlights the need for greater understanding of outcomes associated with subsequent treatment choices and potential benefits of switching.
一些使用肿瘤坏死因子抑制剂(TNFi)的类风湿关节炎(RA)患者疗效不佳或耐受性差,因此转而使用另一种TNFi(换药循环)或采用另一种作用方式的治疗方法(换药)。本研究调查了美国RA患者的特征、处方模式和治疗实践。
数据来自阿德尔菲特定疾病项目(2016年第二季度至第三季度)。风湿病学家为接受过≥1种靶向治疗的成年RA患者填写了一份调查问卷和患者记录表。患者按首次使用的靶向治疗类别以及单药治疗与联合治疗进行分组。接受过≥1种靶向治疗的TNFi患者被分类为换药循环者或换药者。单因素分析比较了各分析组的患者特征和医生因素。
总体而言,631例患者接受了≥1种靶向治疗;535例患者首次接受TNFi靶向治疗,53例接受非TNFi生物改善病情抗风湿药(bDMARD)治疗,43例接受托法替布治疗。在577例已知传统合成(cs)DMARD使用情况的患者中,18.7%接受单药治疗,81.3%接受联合治疗。联合治疗患者在开始首次靶向治疗前接受的伴随用药显著多于单药治疗患者(P<0.05)。医生开出首次靶向治疗处方的首要原因是总体疗效显著(79.9%)。在163例接受第二种靶向治疗的患者中,60.7%为换药循环者。与换药者相比,换药循环者坚持首次靶向治疗的比例较低(P=0.03)。医生在这一阶段换药的主要原因是病情恶化(46.6%)。
大多数患者首次接受TNFi靶向治疗;超过半数随后换药循环至另一种TNFi。这表明其他因素可能影响第二次靶向治疗的选择,并突出了更深入了解后续治疗选择相关结果以及换药潜在益处的必要性。