Department of Emergency, Beijing Chao-Yang Hospital, Capital Medical University, No.5 Jingyuan Road, Shijingshan District, Beijing, 100048, P.R. China.
BMC Infect Dis. 2020 Apr 29;20(1):316. doi: 10.1186/s12879-020-05044-0.
The study aimed to investigate the predictive value of the quick sequential organ failure assessment (qSOFA) for clinical outcomes in emergency patients with community-acquired pneumonia (CAP).
A total of 742 CAP cases from the emergency department (ED) were enrolled in this study. The scoring systems including the qSOFA, SOFA and CURB-65 (confusion, urea, respiratory rate, blood pressure and age) were used to predict the prognostic outcomes of CAP in ICU-admission, acute respiratory distress syndrome (ARDS) and 28-day mortality. According to the area under the curve (AUC) of the receiver operating characteristic (ROC) curves, the accuracies of prediction of the scoring systems were analyzed among CAP patients.
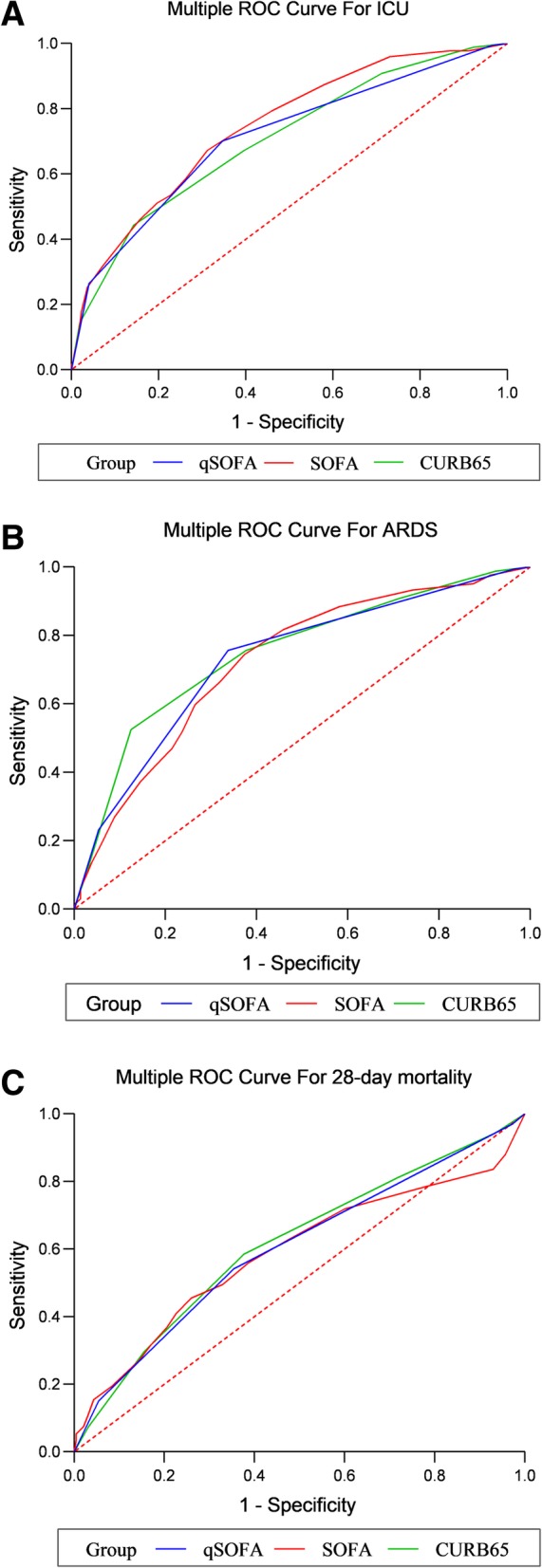
The AUC values of the qSOFA, SOFA and CURB-65 scores for ICU-admission among CAP patients were 0.712 (95%CI: 0.678-0.745, P < 0.001), 0.744 (95%CI: 0.711-0.775, P < 0.001) and 0.705 (95%CI: 0.671-0.738, P < 0.001), respectively. For ARDS, the AUC values of the qSOFA, SOFA and CURB-65 scores were 0.730 (95%CI: 0.697-0.762, P < 0.001), 0.724 (95%CI: 0.690-0.756, P < 0.001) and 0.749 (95%CI: 0.716-0.780, P < 0.001), respectively. After 28 days of follow-up, the AUC values of the qSOFA, SOFA and CURB-65 scores for 28-day mortality were 0.602 (95%CI: 0.566-0.638, P < 0.001), 0.587 (95%CI: 0.551-0.623, P < 0.001) and 0.614 (95%CI: 0.577-0.649, P < 0.001) in turn. There were no statistical differences between qSOFA and SOFA scores for predicting ICU-admission (Z = 1.482, P = 0.138), ARDS (Z = 0.321, P = 0.748) and 28-day mortality (Z = 0.573, P = 0.567). Moreover, we found no differences to predict the ICU-admission (Z = 0.370, P = 0.712), ARDS (Z = 0.900, P = 0.368) and 28-day mortality (Z = 0.768, P = 0.442) using qSOFA or CURB-65 scores.
qSOFA was not inferior to SOFA or CURB-65 scores in predicting the ICU-admission, ARDS and 28-day mortality of patients presenting in the ED with CAP.
本研究旨在探讨快速序贯器官衰竭评估(qSOFA)对社区获得性肺炎(CAP)急诊患者临床结局的预测价值。
本研究纳入了急诊科(ED)的 742 例 CAP 病例。使用 qSOFA、SOFA 和 CURB-65(意识障碍、尿素、呼吸频率、血压和年龄)评分系统来预测 CAP 患者 ICU 入住、急性呼吸窘迫综合征(ARDS)和 28 天死亡率的预后结局。根据受试者工作特征(ROC)曲线的曲线下面积(AUC),分析评分系统在 CAP 患者中的预测准确性。
qSOFA、SOFA 和 CURB-65 评分预测 CAP 患者 ICU 入住的 AUC 值分别为 0.712(95%CI:0.678-0.745,P<0.001)、0.744(95%CI:0.711-0.775,P<0.001)和 0.705(95%CI:0.671-0.738,P<0.001)。对于 ARDS,qSOFA、SOFA 和 CURB-65 评分的 AUC 值分别为 0.730(95%CI:0.697-0.762,P<0.001)、0.724(95%CI:0.690-0.756,P<0.001)和 0.749(95%CI:0.716-0.780,P<0.001)。经过 28 天的随访,qSOFA、SOFA 和 CURB-65 评分预测 28 天死亡率的 AUC 值分别为 0.602(95%CI:0.566-0.638,P<0.001)、0.587(95%CI:0.551-0.623,P<0.001)和 0.614(95%CI:0.577-0.649,P<0.001)。qSOFA 与 SOFA 评分预测 ICU 入住(Z=1.482,P=0.138)、ARDS(Z=0.321,P=0.748)和 28 天死亡率(Z=0.573,P=0.567)的差异无统计学意义。此外,我们发现 qSOFA 或 CURB-65 评分预测 ICU 入住(Z=0.370,P=0.712)、ARDS(Z=0.900,P=0.368)和 28 天死亡率(Z=0.768,P=0.442)的差异也无统计学意义。
qSOFA 在预测 ED 中 CAP 患者的 ICU 入住、ARDS 和 28 天死亡率方面并不逊于 SOFA 或 CURB-65 评分。