Russell Clark D, Baillie J Kenneth
Roslin Institute, University of Edinburgh, Midlothian EH25 9RG, UK.
Intensive Care Unit, Royal Infirmary of Edinburgh, Edinburgh EH16 4SA, UK.
Curr Opin Syst Biol. 2017 Apr;2:140-146. doi: 10.1016/j.coisb.2017.04.003. Epub 2017 Apr 27.
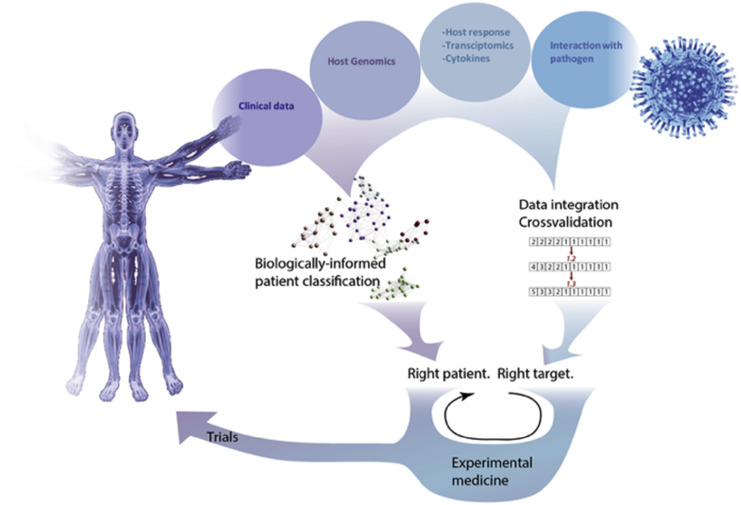
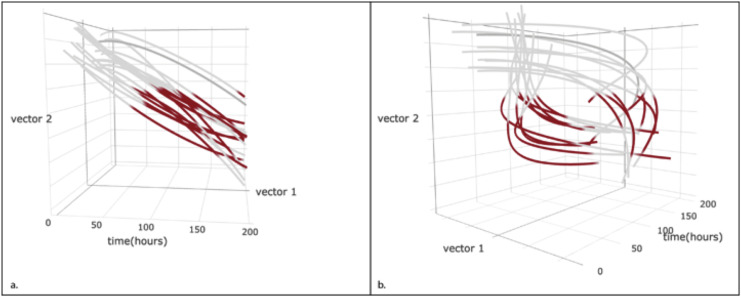
Among the many medical applications of systems biology, we contend that infectious disease is one of the most important and tractable targets. We take the view that the complexity of the immune system is an inevitable consequence of its evolution, and this complexity has frustrated reductionist efforts to develop host-directed therapies for infection. However, since hosts vary widely in susceptibility and tolerance to infection, host-directed therapies are likely to be effective, by altering the biology of a susceptible host to induce a response more similar to a host who survives. Such therapies should exert minimal selection pressure on organisms, thus greatly decreasing the probability of pathogen resistance developing. A systems medicine approach to infection has the potential to provide new solutions to old problems: to identify host traits that are potentially amenable to therapeutic intervention, and the host immune factors that could be targeted by host-directed therapies. Furthermore, undiscovered sub-groups with different responses to treatment are almost certain to exist among patients presenting with life-threatening infection, since this population is markedly clinically heterogeneous. A major driving force behind high-throughput clinical phenotyping studies is the aspiration that these subgroups, hitherto opaque to observation, may be observed in the data generated by new technologies. Subgroups of patients are unlikely to be static - serial clinical and biological phenotyping may reveal different trajectories through the pathophysiology of disease, in which different therapeutic approaches are required. We suggest there are two major goals for systems biology in infection medicine: (1) to identify subgroups of patients that share treatable features; and, (2) to integrate high-throughput data from clinical and sources in order to predict tractable therapeutic targets with the potential to alter disease trajectories for individual patients.
在系统生物学的众多医学应用中,我们认为传染病是最重要且易于处理的目标之一。我们认为,免疫系统的复杂性是其进化的必然结果,而这种复杂性使得开发针对感染的宿主导向疗法的还原论努力受挫。然而,由于宿主对感染的易感性和耐受性差异很大,宿主导向疗法通过改变易感宿主的生物学特性以诱导更类似于存活宿主的反应,可能会有效。此类疗法应对生物体施加最小的选择压力,从而大大降低病原体产生耐药性的可能性。一种针对感染的系统医学方法有可能为老问题提供新的解决方案:识别可能适合进行治疗干预的宿主特征,以及宿主导向疗法可靶向的宿主免疫因子。此外,在患有危及生命感染的患者中几乎肯定存在对治疗反应不同的未被发现的亚组,因为这一人群在临床上具有明显的异质性。高通量临床表型研究背后的一个主要驱动力是期望在新技术产生的数据中观察到这些迄今为止难以观察到的亚组。患者亚组不太可能是静态的——连续的临床和生物学表型研究可能会揭示疾病病理生理学中的不同轨迹,其中需要不同的治疗方法。我们认为感染医学中的系统生物学有两个主要目标:(1)识别具有可治疗特征的患者亚组;(2)整合来自临床和其他来源的高通量数据,以便预测有可能改变个体患者疾病轨迹的可处理治疗靶点。