Department of Otolaryngology-Head & Neck Surgery, Indiana University, Indianapolis, Indiana, USA.
Department of Otolaryngology-Head & Neck Surgery, Cedars Sinai, Los Angeles, California, USA.
Otolaryngol Head Neck Surg. 2020 Jul;163(1):145-150. doi: 10.1177/0194599820929274. Epub 2020 May 19.
The primary mode of viral transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is thought to occur through the spread of respiratory droplets. The objective of this study was to investigate droplet and splatter patterns resulting from common endoscopic endonasal procedures.
Cadaver simulation series.
Dedicated surgical laboratory.
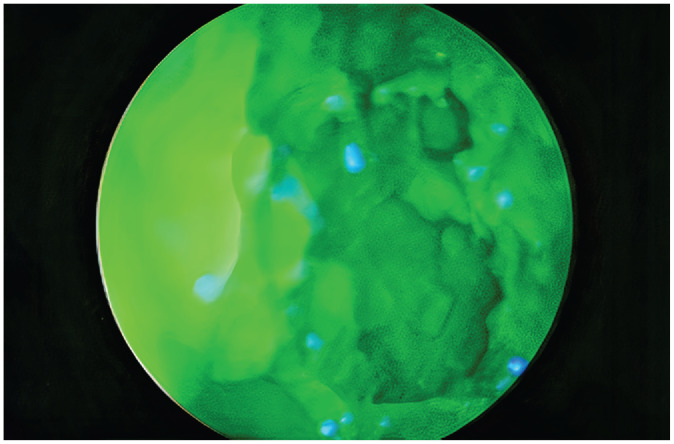
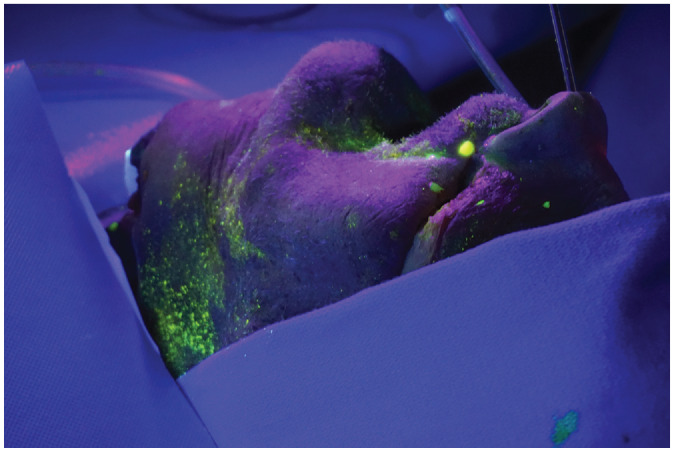
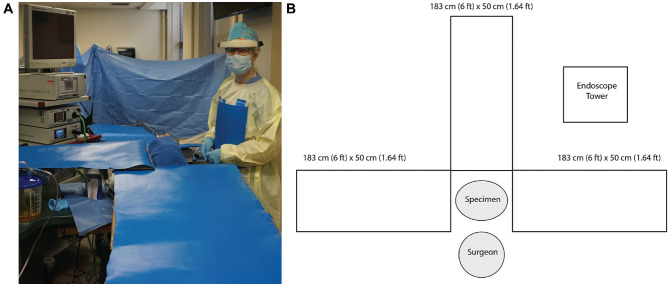
After instilling cadaver head specimens (n = 2) with fluorescein solution, endoscopic endonasal procedures were systematically performed to evaluate the quantity, size, and distance of droplets and splatter following each experimental condition.
There were no observable fluorescein droplets or splatter noted in the measured surgical field in any direction after nasal endoscopy, septoplasty with microdebrider-assisted turbinoplasty, cold-steel functional endoscopic sinus surgery (FESS), and all experimental conditions using an ultrasonic aspirator. Limited droplet spread was noted with microdebrider FESS (2 droplets, <1 mm in size, within 10 cm), drilling of the sphenoid rostrum with a diamond burr (8, <1 mm, 12 cm), and drilling of the frontal beak with a cutting burr (5, <1 mm, 9 cm); however, the use of concurrent suction while drilling resulted in no droplets or splatter. The control condition of external activation of the drill resulted in gross contamination (11, 2 cm, 13 cm).
Our results indicate that there is very little droplet generation from routine rhinologic procedures. The droplet generation from drilling was mitigated with the use of concurrent suction. Extreme caution should be used to avoid activating powered instrumentation outside of the nasal cavity, which was found to cause droplet contamination.
严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)的主要病毒传播方式被认为是通过呼吸道飞沫传播。本研究旨在调查常见鼻内镜鼻窦内手术引起的飞沫和溅出模式。
尸体模拟系列。
专用手术实验室。
在向尸体头部标本(n=2)中注入荧光溶液后,系统地进行鼻内镜鼻窦内手术,以评估每种实验条件后飞沫和溅出物的数量、大小和距离。
在鼻内镜、鼻中隔成形术联合微钻辅助鼻甲切除术、冷刀功能性鼻窦手术(FESS)以及所有使用超声吸引器的实验条件下,在任何方向的测量手术区域均未观察到可见的荧光液滴或溅出物。微钻 FESS(2 滴,<1mm 大小,<10cm)、钻石磨钻钻凿蝶骨前颅底(8 滴,<1mm,12cm)和切割磨钻钻凿额喙(5 滴,<1mm,9cm)时仅观察到有限的飞沫扩散;但在钻孔时同时使用抽吸可防止飞沫或溅出物产生。使用外部驱动钻时的对照条件会导致严重污染(11 滴,2cm,13cm)。
我们的结果表明,常规鼻科手术产生的飞沫很少。使用同时抽吸可减轻钻孔时产生的飞沫。应格外小心,避免在鼻腔外激活电动仪器,因为这会导致飞沫污染。