Department of Microbiology, Queen Mary Hospital, Hong Kong Special Administrative Region, China; Infection Control Team, Queen Mary Hospital, Hong Kong West Cluster, Hong Kong Special Administrative Region, China.
Infection Control Team, Queen Mary Hospital, Hong Kong West Cluster, Hong Kong Special Administrative Region, China.
Am J Infect Control. 2020 Aug;48(8):890-896. doi: 10.1016/j.ajic.2020.05.018. Epub 2020 May 24.
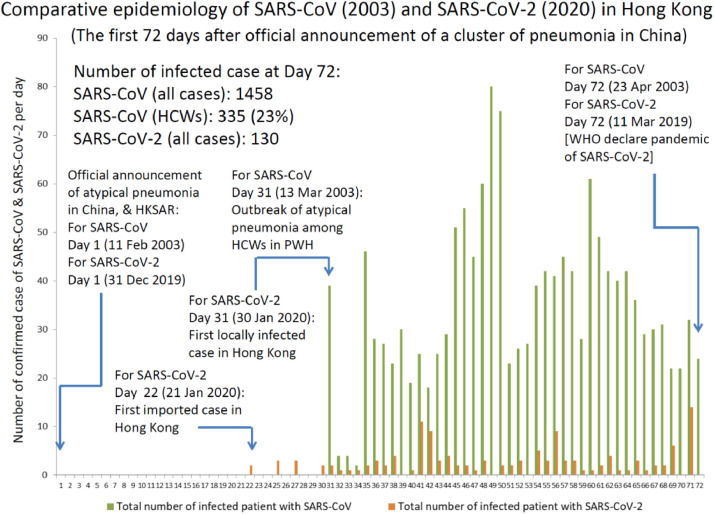
To describe the infection control strategy to achieve zero nosocomial transmission of symptomatic coronavirus disease (COVID-19) due to SARS-CoV-2 during the prepandemic phase (the first 72 days after announcement of pneumonia cases in Wuhan) in Hong Kong.
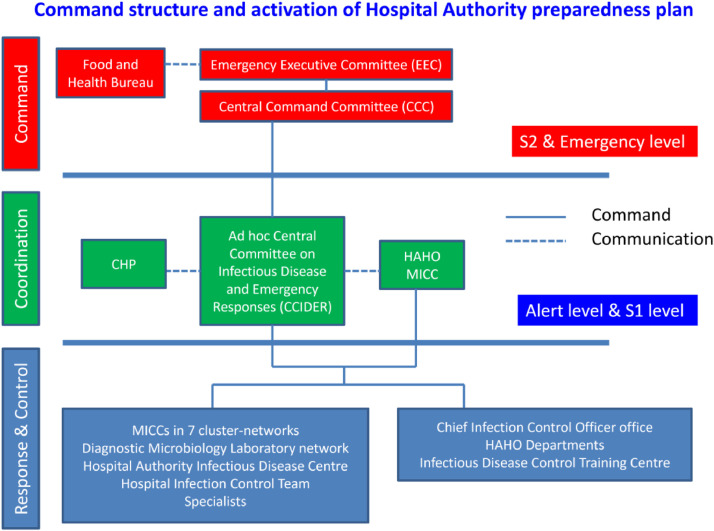
Administrative support with the aim of zero nosocomial transmission by reducing elective clinical services, decanting wards, mobilizing isolation facilities, providing adequate personal protective equipment, coordinating laboratory network for rapid molecular diagnosis under 4-tier active surveillance for hospitalized patients and outpatients, and organizing staff forum and training was implemented under the framework of preparedness plan in Hospital Authority. The trend of SARS-CoV-2 in the first 72 days was compared with that of SARS-CoV 2003.
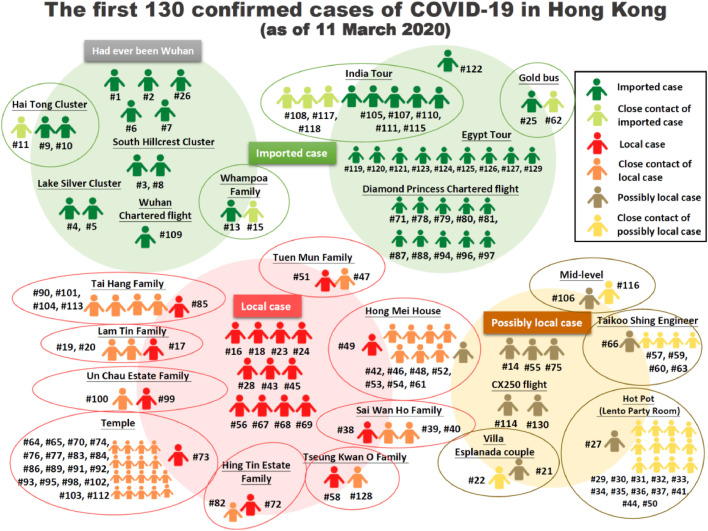
Up to day 72 of the epidemic, 130 (0.40%) of 32,443 patients being screened confirmed to have SARS-CoV-2 by reverse transcription polymerase chain reaction. Compared with SARS outbreak in 2003, the SARS-CoV-2 case load constituted 8.9% (130 SARS-CoV-2/1458 SARS-CoV) of SARS-CoV infected cases at day 72 of the outbreak. The incidences of nosocomial acquisition of SARS-CoV per 1,000 SARS-patient-day and per 100 SARS-patient-admission were 7.9 and 16.9, respectively, which were significantly higher than the corresponding incidences of SARS-CoV-2 (zero infection, P <.001).
Administrative support to infection control could minimize the risk of nosocomial transmission of SARS-CoV-2.
描述在香港大流行前阶段(武汉宣布出现肺炎病例后的头 72 天),为实现零院内传播有症状的 2019 冠状病毒病(COVID-19),针对严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)而采取的感染控制策略。
医管局在准备计划框架下,实施行政支援,以达到零院内传播的目标,包括减少非紧急临床服务、转科、调动隔离设施、提供足够的个人防护装备、协调医院病人和门诊病人的四级主动监测下的快速分子诊断实验室网络,以及组织员工论坛和培训。对 SARS-CoV-2 于前 72 天的趋势与 2003 年 SARS-CoV 的趋势进行了比较。
在疫情暴发的第 72 天,对 32443 名接受筛查的患者中,有 130 名(0.40%)经逆转录聚合酶链反应证实携带 SARS-CoV-2。与 2003 年 SARS 暴发相比,SARS-CoV-2 病例占暴发第 72 天 SARS-CoV 感染者的 8.9%(130 例 SARS-CoV-2/1458 例 SARS-CoV)。每 1000 个 SARS 患者日和每 100 个 SARS 患者入院的 SARS-CoV 院内获得发生率分别为 7.9 和 16.9,明显高于 SARS-CoV-2(零感染,P<0.001)。
感染控制的行政支援可最大程度降低 SARS-CoV-2 院内传播的风险。