Department of Microbiology, Queen Mary Hospital, Hong Kong Special Administrative Region, China.
Infection Control Team, Queen Mary Hospital, Hong Kong West Cluster, Hong Kong Special Administrative Region, China.
Infect Control Hosp Epidemiol. 2020 May;41(5):493-498. doi: 10.1017/ice.2020.58. Epub 2020 Mar 5.
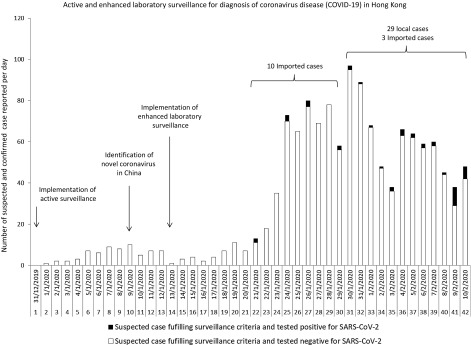
To describe the infection control preparedness measures undertaken for coronavirus disease (COVID-19) due to SARS-CoV-2 (previously known as 2019 novel coronavirus) in the first 42 days after announcement of a cluster of pneumonia in China, on December 31, 2019 (day 1) in Hong Kong.
A bundled approach of active and enhanced laboratory surveillance, early airborne infection isolation, rapid molecular diagnostic testing, and contact tracing for healthcare workers (HCWs) with unprotected exposure in the hospitals was implemented. Epidemiological characteristics of confirmed cases, environmental samples, and air samples were collected and analyzed.
From day 1 to day 42, 42 of 1,275 patients (3.3%) fulfilling active (n = 29) and enhanced laboratory surveillance (n = 13) were confirmed to have the SARS-CoV-2 infection. The number of locally acquired case significantly increased from 1 of 13 confirmed cases (7.7%, day 22 to day 32) to 27 of 29 confirmed cases (93.1%, day 33 to day 42; P < .001). Among them, 28 patients (66.6%) came from 8 family clusters. Of 413 HCWs caring for these confirmed cases, 11 (2.7%) had unprotected exposure requiring quarantine for 14 days. None of these was infected, and nosocomial transmission of SARS-CoV-2 was not observed. Environmental surveillance was performed in the room of a patient with viral load of 3.3 × 106 copies/mL (pooled nasopharyngeal and throat swabs) and 5.9 × 106 copies/mL (saliva), respectively. SARS-CoV-2 was identified in 1 of 13 environmental samples (7.7%) but not in 8 air samples collected at a distance of 10 cm from the patient's chin with or without wearing a surgical mask.
Appropriate hospital infection control measures was able to prevent nosocomial transmission of SARS-CoV-2.
描述 2019 年 12 月 31 日(第 1 天)在中国宣布发生一组肺炎后,在香港对 2019 年新型冠状病毒(SARS-CoV-2,此前称为 2019 年新型冠状病毒)引起的冠状病毒病(COVID-19)所采取的感染控制准备措施。
实施了主动和强化实验室监测、早期空气传播感染隔离、快速分子诊断检测以及对医院内无保护暴露的医护人员(HCW)进行接触者追踪的综合方法。收集和分析了确诊病例、环境样本和空气样本的流行病学特征。
从第 1 天到第 42 天,在满足主动(n=29)和强化实验室监测(n=13)的 1275 名患者中,有 42 名(3.3%)被确认为 SARS-CoV-2 感染。本地获得性病例的数量从第 22 天至第 32 天的 13 例确诊病例中的 1 例(7.7%)显著增加到第 33 天至第 42 天的 29 例确诊病例中的 27 例(93.1%;P<.001)。其中,28 例(66.6%)患者来自 8 个家庭集群。在照顾这些确诊患者的 413 名 HCW 中,有 11 名(2.7%)无保护暴露,需要隔离 14 天。这些人中没有一个被感染,也没有观察到 SARS-CoV-2 的医院内传播。对病毒载量分别为 3.3×106 拷贝/mL(鼻咽和咽拭子混合)和 5.9×106 拷贝/mL(唾液)的一名患者的房间进行了环境监测。在 13 份环境样本中的 1 份(7.7%)中发现了 SARS-CoV-2,但在距离患者下巴 10 厘米处采集的 8 份空气样本中未发现 SARS-CoV-2,这些空气样本采集时患者或佩戴或未佩戴外科口罩。
适当的医院感染控制措施能够防止 SARS-CoV-2 的医院内传播。