Department of Population Health, NYU Grossman School of Medicine, New York, NY, USA.
Institute for Disease Modeling, Bellevue, WA, USA.
J Int AIDS Soc. 2020 Jun;23 Suppl 3(Suppl 3):e25527. doi: 10.1002/jia2.25527.
Over one hundred implementation studies of HIV pre-exposure prophylaxis (PrEP) are completed, underway or planned. We synthesized evidence from these studies to inform mathematical modelling of the prevention cascade for oral and long-acting PrEP in the setting of western Kenya, one of the world's most heavily HIV-affected regions.
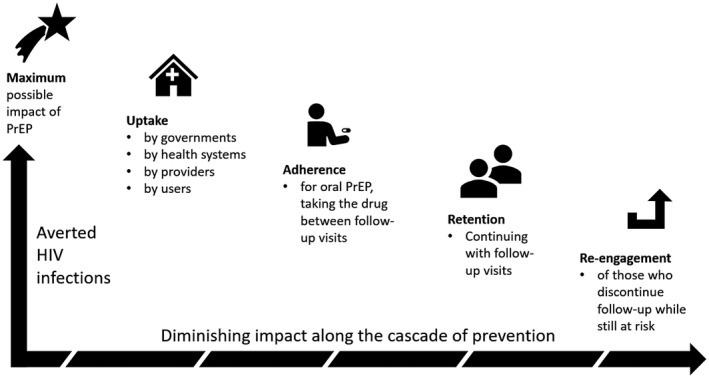
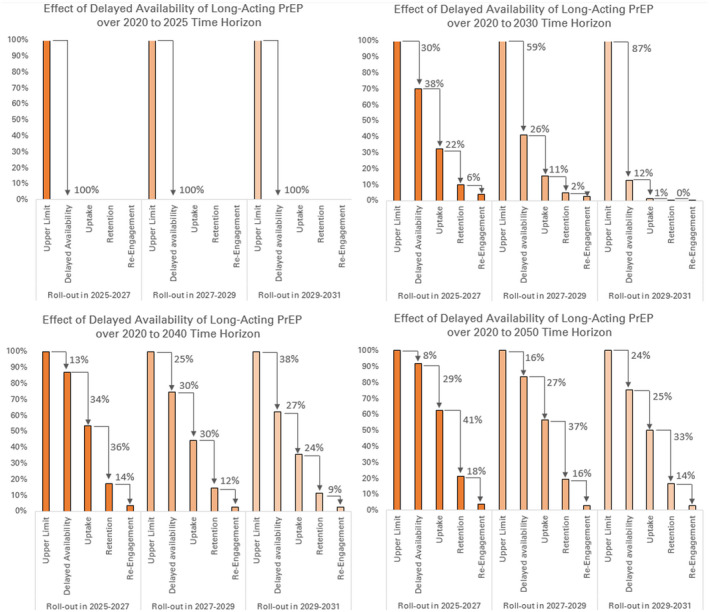
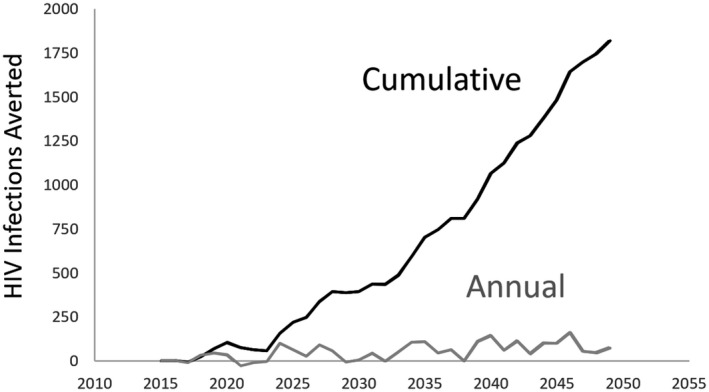
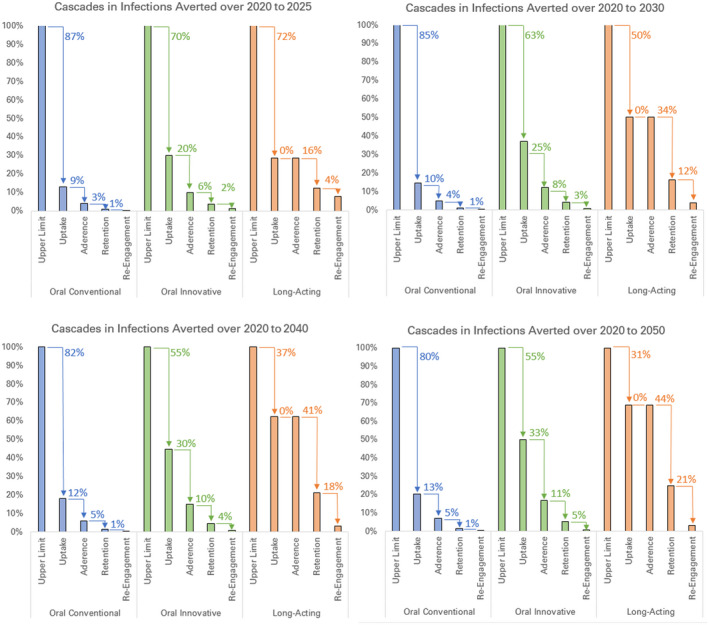
We incorporated steps of the PrEP prevention cascade - uptake, adherence, retention and re-engagement after discontinuation - into EMOD-HIV, an open-source transmission model calibrated to the demography and HIV epidemic patterns of western Kenya. Early PrEP implementation research from East Africa was used to parameterize prevention cascades for oral PrEP as currently implemented, delivery innovations for oral PrEP, and future long-acting PrEP. We compared infections averted by PrEP at the population level for different cascade assumptions and sub-populations on PrEP. Analyses were conducted over the 2020 to 2040 time horizon, with additional sensitivity analyses for the time horizon of analysis and the time when long-acting PrEP becomes available.
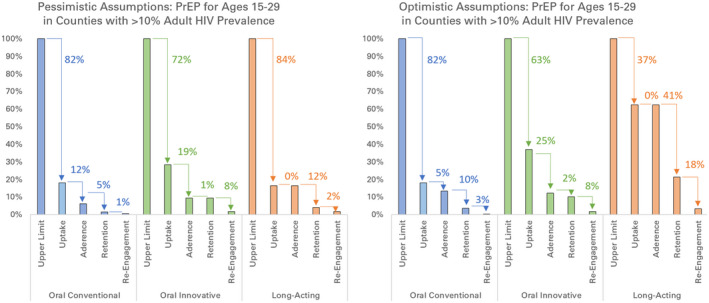
The maximum impact of oral PrEP diminished by over 98% across all prevention cascades, with the exception of long-acting PrEP under optimistic assumptions about uptake and re-engagement after discontinuation. Long-acting PrEP had the highest population-level impact, even after accounting for possible delays in product availability, primarily because its effectiveness does not depend on drug adherence. Retention was the most significant cascade step reducing the potential impact of long-acting PrEP. These results were robust to assumptions about the sub-populations receiving PrEP, but were highly influenced by assumptions about re-initiation of PrEP after discontinuation, about which evidence was sparse.
Implementation challenges along the prevention cascade compound to diminish the population-level impact of oral PrEP. Long-acting PrEP is expected to be less impacted by user uptake and adherence, but it is instead dependent on product availability in the short term and retention in the long term. To maximize the impact of long-acting PrEP, ensuring timely product approval and rollout is critical. Research is needed on strategies to improve retention and patterns of PrEP re-initiation.
目前已有超过 100 项关于艾滋病毒暴露前预防 (PrEP) 的实施研究完成、正在进行或计划进行。我们综合了这些研究的证据,为在肯尼亚西部(世界上受艾滋病毒影响最严重的地区之一)建立口服和长效 PrEP 预防级联模型提供信息。
我们将 PrEP 预防级联的各个步骤(包括接受、坚持、停药后重新参与)纳入到 EMOD-HIV 中,这是一个根据肯尼亚西部的人口统计学和艾滋病毒流行模式校准的开源传播模型。东非早期的 PrEP 实施研究用于为目前实施的口服 PrEP、口服 PrEP 的交付创新和未来的长效 PrEP 制定预防级联参数。我们比较了不同级联假设和接受 PrEP 的亚人群在人群层面上预防感染的效果。分析在 2020 年至 2040 年的时间范围内进行,并对分析时间范围和长效 PrEP 可用时间进行了额外的敏感性分析。
除了在停药后重新参与和接受方面的假设较为乐观的情况下,长效 PrEP 之外,所有预防级联中,口服 PrEP 的最大影响减少了 98% 以上。即使考虑到产品供应可能存在延迟,长效 PrEP 对人群的影响也最大,这主要是因为其有效性不依赖于药物的坚持使用。保留是减少长效 PrEP 潜在影响的最重要的级联步骤。这些结果对于接受 PrEP 的亚人群的假设是稳健的,但受到停药后重新开始 PrEP 的假设的影响很大,而关于这方面的证据很少。
预防级联中的实施挑战加剧,降低了口服 PrEP 的人群层面的影响。长效 PrEP 预计不会受到使用者接受和坚持使用的影响,但短期内依赖于产品的供应,长期则依赖于保留率。为了最大限度地发挥长效 PrEP 的作用,确保及时批准和推出产品至关重要。需要研究提高保留率和 PrEP 重新启动模式的策略。