Department of Medicine, University of Toronto, Toronto, ON, Canada
Institute for Clinical Evaluative Sciences (ICES), Toronto and Ottawa, ON, Canada.
BMJ. 2020 Jul 6;370:m2257. doi: 10.1136/bmj.m2257.
To measure the associations between newly initiated palliative care in the last six months of life, healthcare use, and location of death in adults dying from non-cancer illness, and to compare these associations with those in adults who die from cancer at a population level.
Population based matched cohort study.
Ontario, Canada between 2010 and 2015.
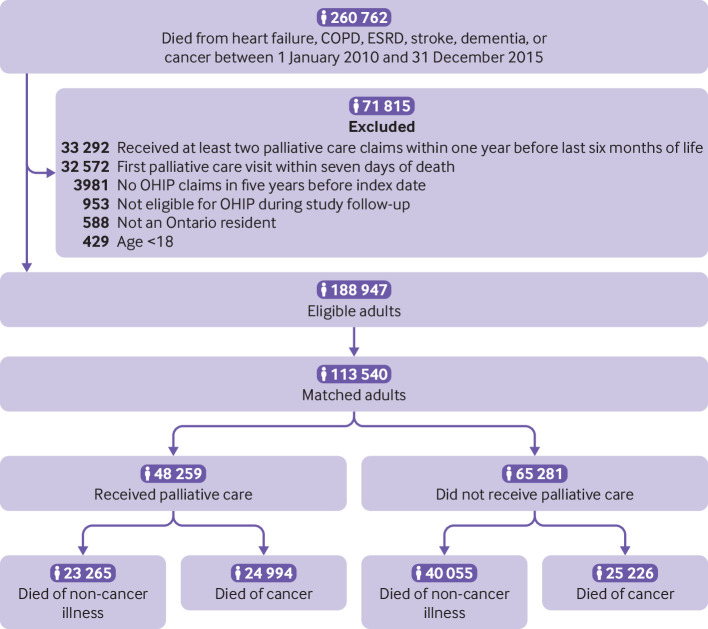
113 540 adults dying from cancer and non-cancer illness who were given newly initiated physician delivered palliative care in the last six months of life administered across all healthcare settings. Linked health administrative data were used to directly match patients on cause of death, hospital frailty risk score, presence of metastatic cancer, residential location (according to 1 of 14 local health integration networks that organise all healthcare services in Ontario), and a propensity score to receive palliative care that was derived by using age and sex.
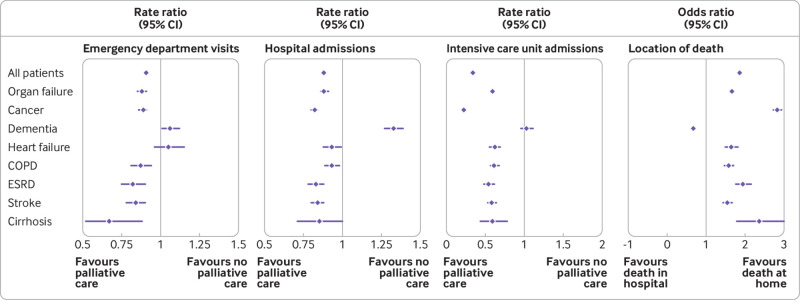
Rates of emergency department visits, admissions to hospital, and admissions to the intensive care unit, and odds of death at home versus in hospital after first palliative care visit, adjusted for patient characteristics (such as age, sex, and comorbidities).
In patients dying from non-cancer illness related to chronic organ failure (such as heart failure, cirrhosis, and stroke), palliative care was associated with reduced rates of emergency department visits (crude rate 1.9 (standard deviation 6.2) 2.9 (8.7) per person year; adjusted rate ratio 0.88, 95% confidence interval 0.85 to 0.91), admissions to hospital (crude rate 6.1 (standard deviation 10.2) 8.7 (12.6) per person year; adjusted rate ratio 0.88, 95% confidence interval 0.86 to 0.91), and admissions to the intensive care unit (crude rate 1.4 (standard deviation 5.9) 2.9 (8.7) per person year; adjusted rate ratio 0.59, 95% confidence interval 0.56 to 0.62) compared with those who did not receive palliative care. Additionally increased odds of dying at home or in a nursing home compared with dying in hospital were found in these patients (n=6936 (49.5%) n=9526 (39.6%); adjusted odds ratio 1.67, 95% confidence interval 1.60 to 1.74). Overall, in patients dying from dementia, palliative care was associated with increased rates of emergency department visits (crude rate 1.2 (standard deviation 4.9) 1.3 (5.5) per person year; adjusted rate ratio 1.06, 95% confidence interval 1.01 to 1.12) and admissions to hospital (crude rate 3.6 (standard deviation 8.2) 2.8 (7.8) per person year; adjusted rate ratio 1.33, 95% confidence interval 1.27 to 1.39), and reduced odds of dying at home or in a nursing home (n=6667 (72.1%) n=13 384 (83.5%); adjusted odds ratio 0.68, 95% confidence interval 0.64 to 0.73). However, these rates differed depending on whether patients dying with dementia lived in the community or in a nursing home. No association was found between healthcare use and palliative care for patients dying from dementia who lived in the community, and these patients had increased odds of dying at home.
These findings highlight the potential benefits of palliative care in some non-cancer illnesses. Increasing access to palliative care through sustained investment in physician training and current models of collaborative palliative care could improve end-of-life care, which might have important implications for health policy.
衡量在生命的最后六个月内新启动的姑息治疗与非癌症疾病患者的医疗保健使用和死亡地点之间的关联,并将这些关联与在人群水平上死于癌症的患者进行比较。
基于人群的匹配队列研究。
加拿大安大略省,2010 年至 2015 年。
113540 名在生命的最后六个月内接受新启动的医生提供的姑息治疗的癌症和非癌症疾病患者,姑息治疗是在所有医疗保健环境下提供的。使用链接的健康行政数据直接根据死因、医院脆弱性风险评分、转移性癌症的存在、居住地点(根据组织安大略省所有医疗保健服务的 14 个地方卫生集成网络中的 1 个)和接受姑息治疗的倾向评分进行匹配,该评分是通过使用年龄和性别得出的。
急诊就诊、住院和入住重症监护病房的比率,以及首次姑息治疗就诊后在家中或医院死亡的可能性,调整了患者特征(如年龄、性别和合并症)。
在因慢性器官衰竭(如心力衰竭、肝硬化和中风)相关的非癌症疾病患者中,姑息治疗与急诊就诊率降低相关(粗率 1.9(标准差 6.2) 2.9(8.7)人年;调整后的比率比 0.88,95%置信区间 0.85 至 0.91)、住院率(粗率 6.1(标准差 10.2) 8.7(12.6)人年;调整后的比率比 0.88,95%置信区间 0.86 至 0.91)和入住重症监护病房的比率(粗率 1.4(标准差 5.9) 2.9(8.7)人年;调整后的比率比 0.59,95%置信区间 0.56 至 0.62)与未接受姑息治疗的患者相比。此外,与在医院死亡相比,这些患者在家中或疗养院死亡的可能性增加(n=6936(49.5%)n=9526(39.6%);调整后的优势比 1.67,95%置信区间 1.60 至 1.74)。总体而言,在患有痴呆症的患者中,姑息治疗与急诊就诊率增加相关(粗率 1.2(标准差 4.9) 1.3(5.5)人年;调整后的比率比 1.06,95%置信区间 1.01 至 1.12)和住院率(粗率 3.6(标准差 8.2) 2.8(7.8)人年;调整后的比率比 1.33,95%置信区间 1.27 至 1.39),以及在家中或疗养院死亡的可能性降低(n=6667(72.1%)n=13384(83.5%);调整后的优势比 0.68,95%置信区间 0.64 至 0.73)。然而,这些比率因患有痴呆症的患者是否居住在社区或疗养院而有所不同。在居住在社区的患有痴呆症的患者中,姑息治疗与医疗保健使用之间没有关联,这些患者在家中死亡的可能性增加。
这些发现强调了姑息治疗在某些非癌症疾病中的潜在益处。通过持续投资于医生培训和当前的姑息治疗协作模式,增加姑息治疗的机会,可以改善临终关怀,这可能对卫生政策有重要影响。