Yu Xiangyang, Gao Shugeng, Xue Qi, Tan Fengwei, Gao Yushun, Mao Yousheng, Wang Dali, Zhao Jun, Li Yin, He Jie, Mu Juwei
Department of Thoracic Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China.
Department of Thoracic Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen 518116, China.
J Thorac Dis. 2020 May;12(5):2583-2594. doi: 10.21037/jtd.2020.03.25.
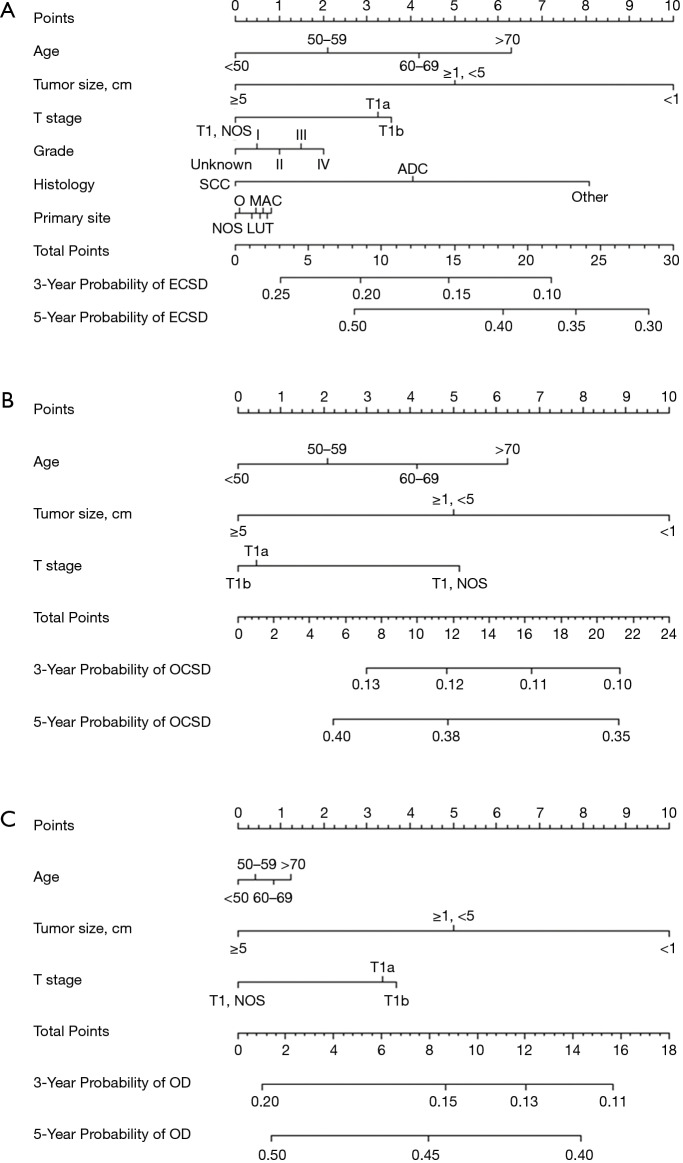
The aim of this population-based study was to perform competing risk analysis and estimate cancer- and other cause-specific mortality in patients who underwent oesophagectomy with pT1N0M0 oesophageal cancer (EC). A competing risks nomogram was also developed to predict the proportional of death from each specific cause.
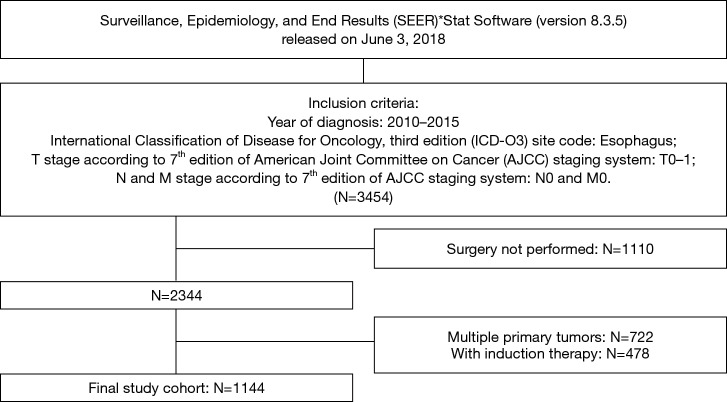
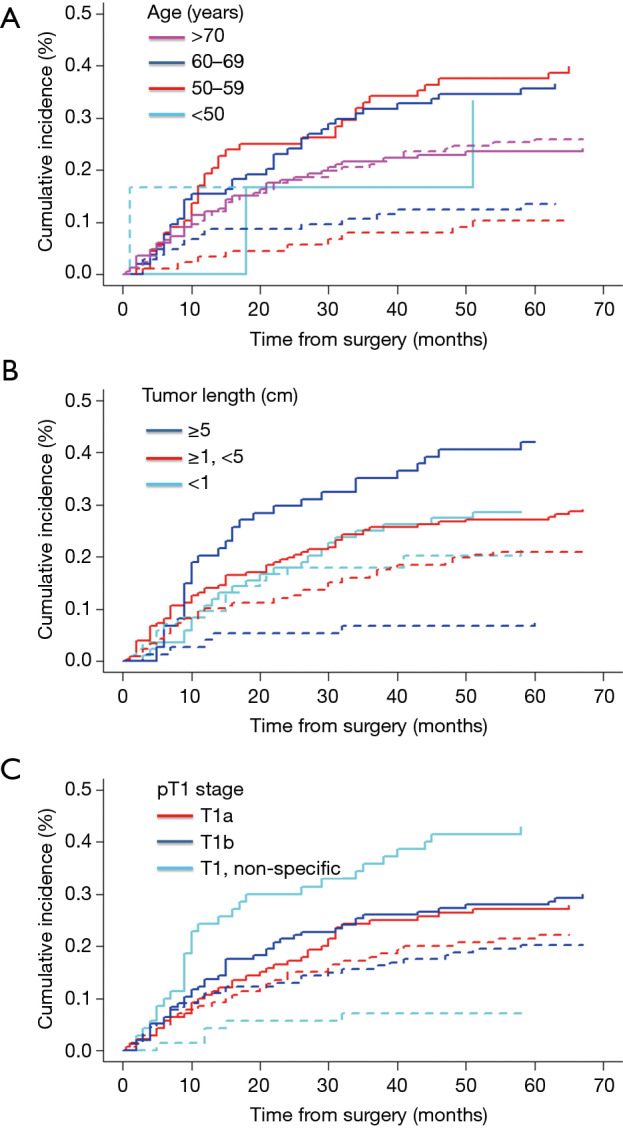
A total of 1,144 patients who received oesophagectomy for pT1N0M0 EC between 2010 and 2015 from SEER database were included. The cumulative incidence function was used to evaluate each cause of death, and the significant difference was assessed by the Grey's test. A nomogram was established using the proportional subdistribution hazard analysis to identify predictors for each cause-specific death.
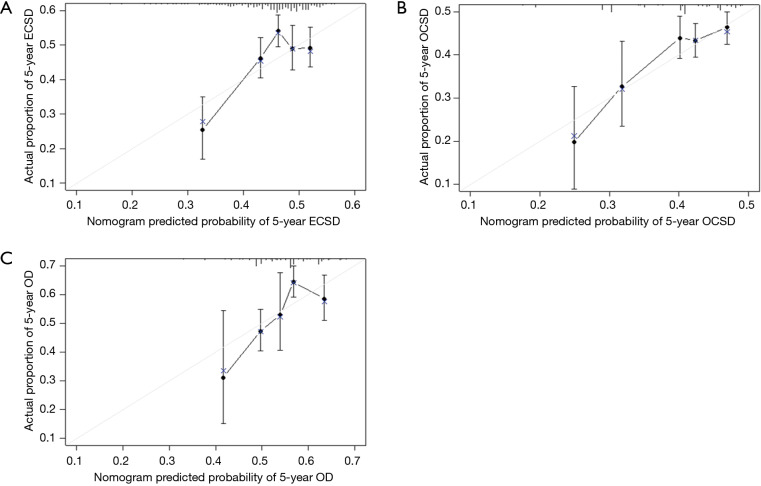
The 5-year cumulative incidence of cancer-specific death for surgically resected pT1N0M0 EC was 15.7%, and the incidence was 11.2% for other cause-specific death. Age, tumour length, pT1 substage, grade, history and primary site were identified as predictive factors for EC-specific death, but only age, tumor length and pT1 substage were associated with death from other cause. Our nomograms showed a relative good discriminative ability, with c-index of 0.663 for the EC-specific mortality model and 0.699 for the other cause-specific mortality model. The calibration curves showed a good match between the nomogram-predicted probabilities and the actual probabilities.
In patients who underwent curative-intent resection for pT1N0M0 EC, death from other causes was an important competing event. During clinical decision making and patient-clinician communication, our quantifiable nomograms could provide a rapid and precise judgement of the risk of death from each cause.
本基于人群的研究旨在进行竞争风险分析,并估计接受 pT1N0M0 食管癌(EC)食管切除术患者的癌症特异性死亡率和其他特定原因死亡率。还开发了一种竞争风险列线图,以预测每种特定原因导致的死亡比例。
纳入 2010 年至 2015 年期间从监测、流行病学和最终结果(SEER)数据库接受 pT1N0M0 EC 食管切除术的 1144 例患者。使用累积发病率函数评估每种死亡原因,并通过 Grey 检验评估显著差异。使用比例子分布风险分析建立列线图,以识别每种特定原因死亡的预测因素。
手术切除的 pT1N0M0 EC 的 5 年癌症特异性死亡累积发病率为 15.7%,其他特定原因死亡的发病率为 11.2%。年龄、肿瘤长度、pT1 亚分期、分级、病史和原发部位被确定为 EC 特异性死亡的预测因素,但只有年龄、肿瘤长度和 pT1 亚分期与其他原因导致的死亡相关。我们的列线图显示出相对良好的判别能力,EC 特异性死亡率模型的 c 指数为 0.663,其他特定原因死亡率模型的 c 指数为 0.699。校准曲线显示列线图预测概率与实际概率之间匹配良好。
在接受 pT1N0M0 EC 根治性切除的患者中,其他原因导致的死亡是一个重要的竞争事件。在临床决策和医患沟通中,我们的可量化列线图可以快速、准确地判断每种原因导致的死亡风险。