Department of Health Promotion, Collegium Medicum, Nicolaus Copernicus University, Curie Skłodowskiej St. 9, 85-094, Bydgoszcz, Poland.
Department of Cardiology and Internal Diseases, Collegium Medicum, Nicolaus Copernicus University, Bydgoszcz, Poland.
Sci Rep. 2020 Jul 21;10(1):12028. doi: 10.1038/s41598-020-68915-1.
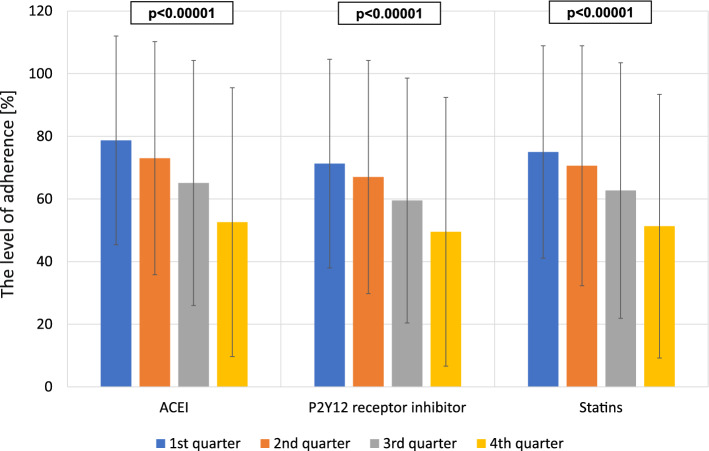
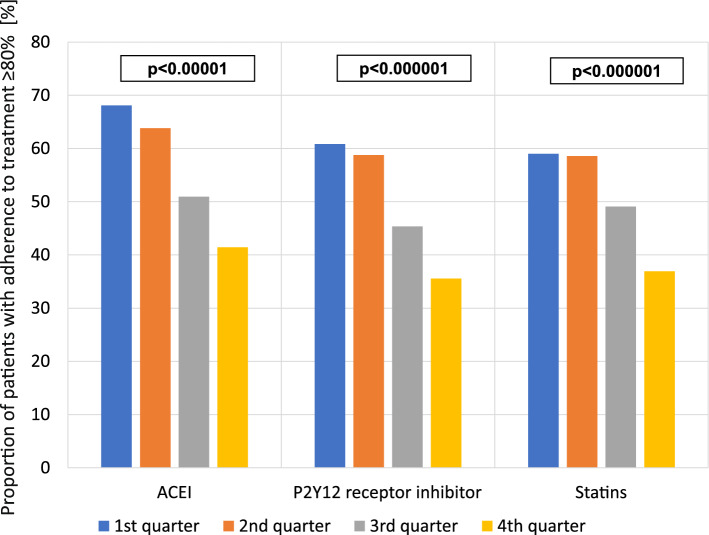
Non-adherence to prescribed medication is a serious limitation of long-term treatment in patients after myocardial infarction (MI), which can be associated with medical, social and economical consequences. Improvement of medication adherence has been shown to be a challenge for healthcare providers. The aim of this study was to evaluate changes in medication adherence and variability of adherence determinants during follow-up in patients after MI. A single-center, cohort observational study was conducted in 225 post-MI patients treated with primary coronary intervention (PCI) (27% women and 73% men) aged 30-91 years. Adherence was defined as availability of evaluated drugs within 1-year after discharge from hospital, based on completed prescriptions data obtained from the National Health Fund. The analysis of therapeutic plan realization (adherence to medication prescribed at discharge from hospital) embraced only reimbursed drugs: ACEIs (ramipril, perindopril), P2Y12 receptor inhibitors (clopidogrel) and statins (atorvastatin, simvastatin, rosuvastatin). Sufficient adherence was defined as ≥ 80%. During 1-year follow-up, adherence for all three drug classes was 64 ± 25%, with 67 ± 32% for ACEIs, 62 ± 34% for P2Y12 receptor inhibitor and 64 ± 32% for statins. A gradual decline in adherence was observed from 65% ± 26% in the first quarter of follow-up to 51% ± 34% in the last quarter of follow-up (p < 0.00001). Sufficient adherence for all drugs classes was found only in 29% of patients throughout the whole follow-up period (44% for ACEI, 36% for P2Y12 receptor inhibitor and 41% for statins). According to a multivariate analysis, age, prior CABG, level of education, place of residence, economic status and marital status were independent predictors of drug adherence. Whereas patients > 65 years and having a history of prior CABG more often had an insufficient adherence to drugs, married and hypertensive patients, city inhabitants and patients with higher education tended to have a sufficient drug adherence. Adherence to pharmacotherapy after myocardial infarction decreases over time in a similar manner for all pivotal groups of drugs prescribed after MI. A number of socioeconomic and clinical factors have been identified to affect medication adherence over time.
不遵医嘱服药是心肌梗死后长期治疗的一个严重限制因素,这可能会导致医疗、社会和经济方面的后果。改善用药依从性一直是医疗保健提供者面临的挑战。本研究旨在评估心肌梗死后患者在随访期间用药依从性的变化和用药依从性决定因素的变化。这是一项单中心、队列观察性研究,纳入了 225 名接受直接经皮冠状动脉介入治疗(PCI)的心肌梗死后患者(27%为女性,73%为男性),年龄为 30-91 岁。根据从国家健康基金获得的完整处方数据,将出院后 1 年内可获得评估药物定义为用药依从性。出院时治疗方案的实现(即服用出院时开具的药物)分析仅纳入报销药物:血管紧张素转换酶抑制剂(赖诺普利、培哚普利)、P2Y12 受体抑制剂(氯吡格雷)和他汀类药物(阿托伐他汀、辛伐他汀、瑞舒伐他汀)。足够的依从性定义为≥80%。在 1 年的随访期间,所有 3 类药物的依从率为 64±25%,血管紧张素转换酶抑制剂为 67±32%,P2Y12 受体抑制剂为 62±34%,他汀类药物为 64±32%。从随访第 1 季度的 65%±26%到第 4 季度的 51%±34%,观察到依从率逐渐下降(p<0.00001)。在整个随访期间,只有 29%的患者所有药物类别的依从率均达到足够水平(血管紧张素转换酶抑制剂为 44%,P2Y12 受体抑制剂为 36%,他汀类药物为 41%)。多变量分析显示,年龄、既往 CABG、教育程度、居住地、经济状况和婚姻状况是药物依从性的独立预测因素。年龄>65 岁和既往 CABG 的患者更常出现药物依从性不足,而已婚和高血压患者、城市居民和受教育程度较高的患者更倾向于药物依从性良好。心肌梗死后,随着时间的推移,所有主要药物组的药物治疗依从性呈相似的下降趋势。一些社会经济和临床因素已被确定会随时间影响药物的依从性。