The DHS Program, ICF, Rockville, MD, USA.
Hubert Department of Global Health, Rollins School of Public Health, Emory University, Atlanta, GA, USA.
Am J Clin Nutr. 2019 Aug 1;112(Suppl 1):458S-467S. doi: 10.1093/ajcn/nqaa141.
Accurate assessment of iron and vitamin A status is needed to inform public health decisions, but most population-level iron and vitamin A biomarkers are independently influenced by inflammation.
We aimed to assess the reproducibility of the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) regression approach to adjust iron [ferritin, soluble transferrin receptor (sTfR)] and vitamin A [retinol-binding protein (RBP), retinol] biomarkers for inflammation (α-1-acid glycoprotein and C-reactive protein).
We conducted a sensitivity analysis comparing unadjusted and adjusted estimates of iron and vitamin A deficiency using the internal-survey regression approach from BRINDA phase 1 (16 surveys in children, 10 surveys in women) and 13 additional surveys for children and women (BRINDA phase 2).
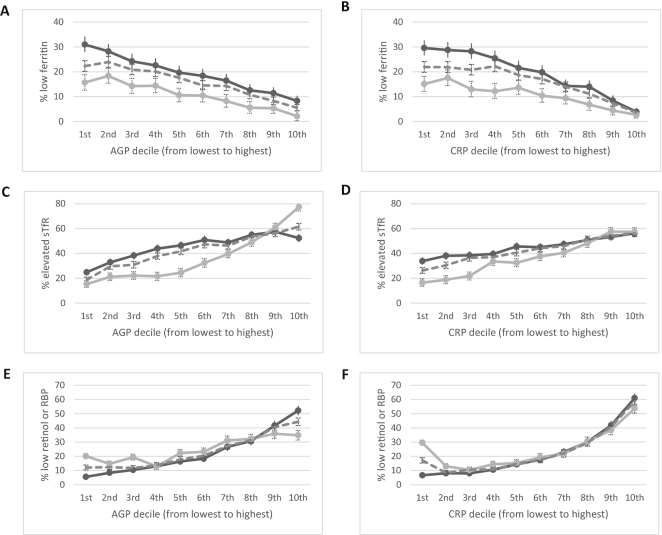
The relations between inflammation and iron or vitamin A biomarkers were statistically significant except for vitamin A biomarkers in women. Heterogeneity of the regression coefficients across surveys was high. Among children, internal-survey adjustments increased the estimated prevalence of depleted iron stores (ferritin <12 µg/L) by a median of 11 percentage points (pp) (24 pp and 9 pp in BRINDA phase 1 and phase 2, respectively), whereas estimates of iron-deficient erythropoiesis (sTfR >8.3 mg/L) decreased by a median of 15 pp (15 pp and 20 pp in BRINDA phase 1 and phase 2, respectively). Vitamin A deficiency (RBP <0.7 µmol/L or retinol <0.7 µmol/L) decreased by a median of 14 pp (18 pp and 8 pp in BRINDA phase 1 and phase 2, respectively) in children. Adjustment for inflammation in women resulted in smaller differences in estimated iron deficiency than in children.
Our findings are consistent with previous BRINDA conclusions that not accounting for inflammation may result in an underestimation of iron deficiency and overestimation of vitamin A deficiency. Research is needed to understand the etiology of the heterogeneity in the regression coefficients before a meta-analyzed regression correction can be considered.
准确评估铁和维生素 A 状况对于公共卫生决策至关重要,但大多数人群水平的铁和维生素 A 生物标志物均受到炎症的独立影响。
我们旨在评估生物标志物反映炎症和营养决定贫血(BRINDA)回归方法调整铁[铁蛋白、可溶性转铁蛋白受体(sTfR)]和维生素 A[视黄醇结合蛋白(RBP)、视黄醇]生物标志物炎症(α-1-酸性糖蛋白和 C 反应蛋白)的重现性。
我们通过 BRINDA 阶段 1(儿童 16 项调查,妇女 10 项调查)和 13 项针对儿童和妇女的额外调查(BRINDA 阶段 2)中的内部调查回归方法,对铁和维生素 A 缺乏症的未调整和调整估计值进行了敏感性分析。
除了妇女的维生素 A 生物标志物外,炎症与铁或维生素 A 生物标志物之间的关系具有统计学意义。各调查之间回归系数的异质性很高。在儿童中,内部调查调整使铁储存耗竭(铁蛋白 <12 µg/L)的估计患病率中位数增加了 11 个百分点(BRINDA 阶段 1 和阶段 2 分别为 24 个百分点和 9 个百分点),而铁缺乏性红细胞生成(sTfR >8.3 mg/L)的估计值中位数降低了 15 个百分点(BRINDA 阶段 1 和阶段 2 分别为 15 个百分点和 20 个百分点)。维生素 A 缺乏症(RBP <0.7 µmol/L 或视黄醇 <0.7 µmol/L)在儿童中中位数降低了 14 个百分点(BRINDA 阶段 1 和阶段 2 分别为 18 个百分点和 8 个百分点)。在妇女中,炎症调整导致铁缺乏症的估计差异小于儿童。
我们的发现与之前 BRINDA 的结论一致,即不考虑炎症可能会导致铁缺乏症的低估和维生素 A 缺乏症的高估。在考虑进行荟萃分析回归校正之前,需要进行研究以了解回归系数异质性的病因。