Immunization Systems Branch, Global Immunization Division, U.S. Centers for Disease Control and Prevention, Atlanta, United States.
Strategic Information and Workforce Development Branch, Global Immunization Division, U.S. Centers for Disease Control and Prevention, Atlanta, United States.
Vaccine. 2020 Sep 3;38(39):6103-6111. doi: 10.1016/j.vaccine.2020.07.031. Epub 2020 Aug 1.
In 2016, the Sierra Leone Ministry of Health and Sanitation (MoHS) piloted VaxTrac, an electronic immunization registry (EIR), in an urban district to improve management of vaccination records and tracking of children who missed scheduled doses. We aimed to document lessons learned to inform decision-making on VaxTrac and similar EIRs' future use.
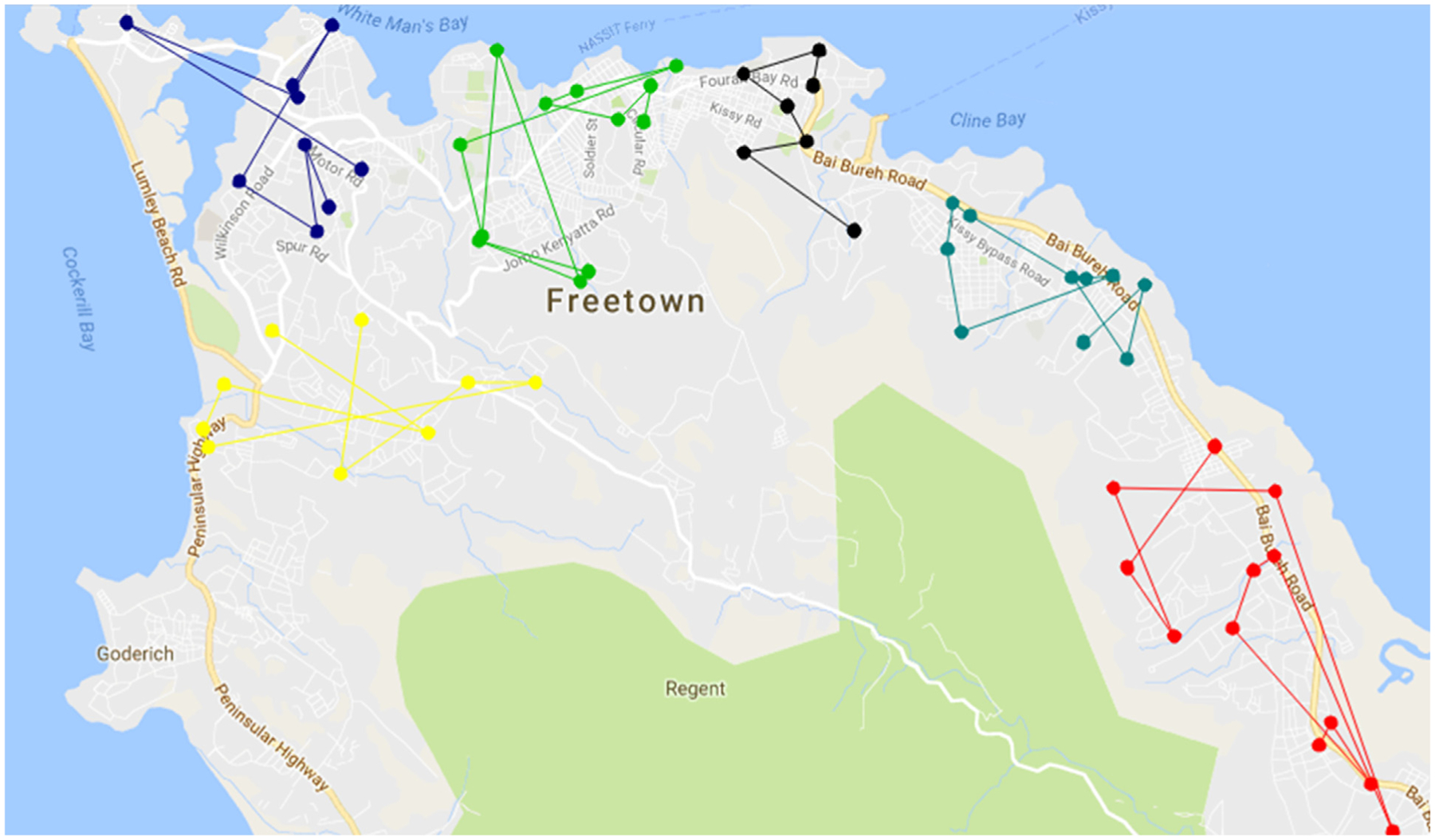
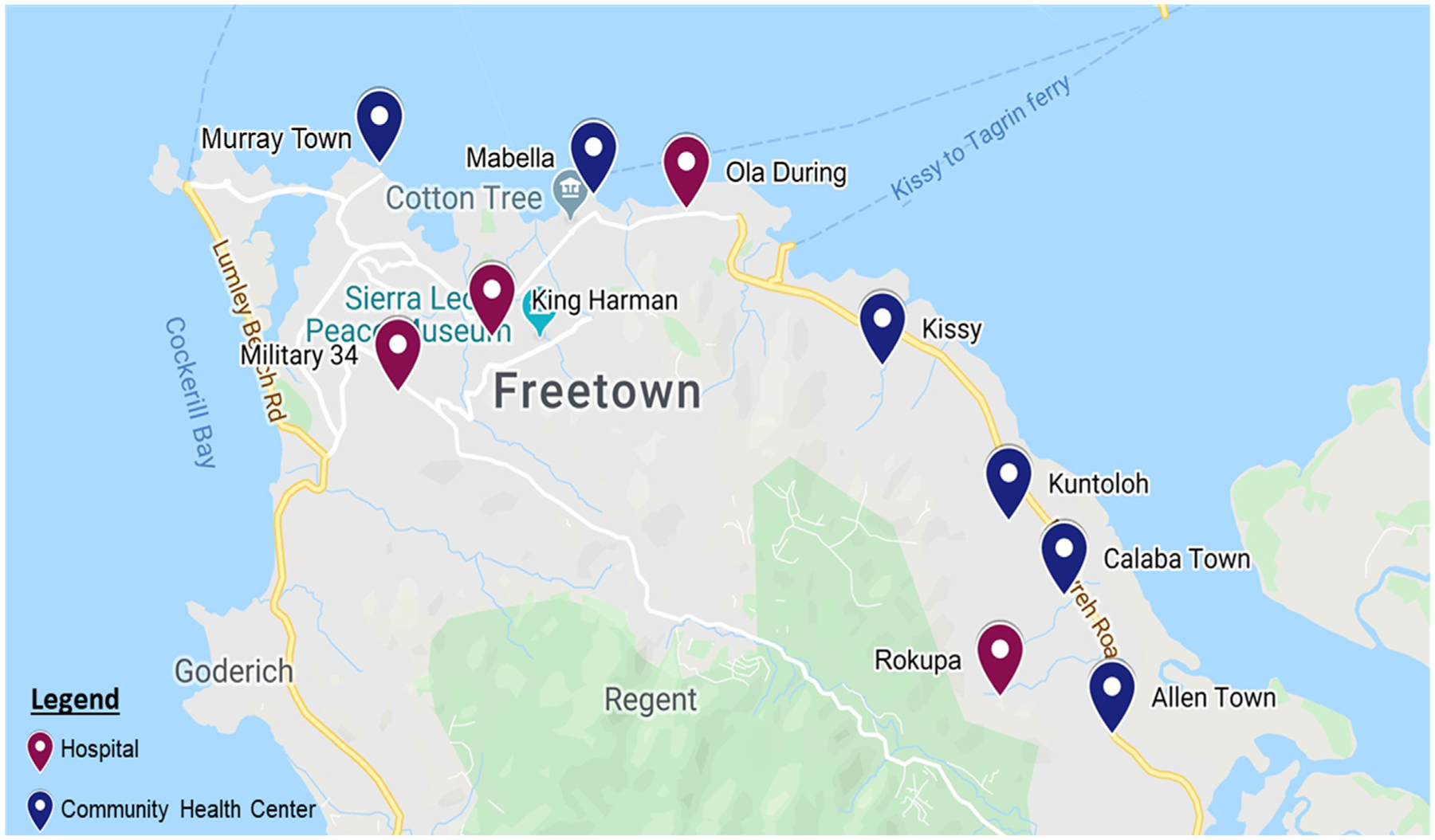
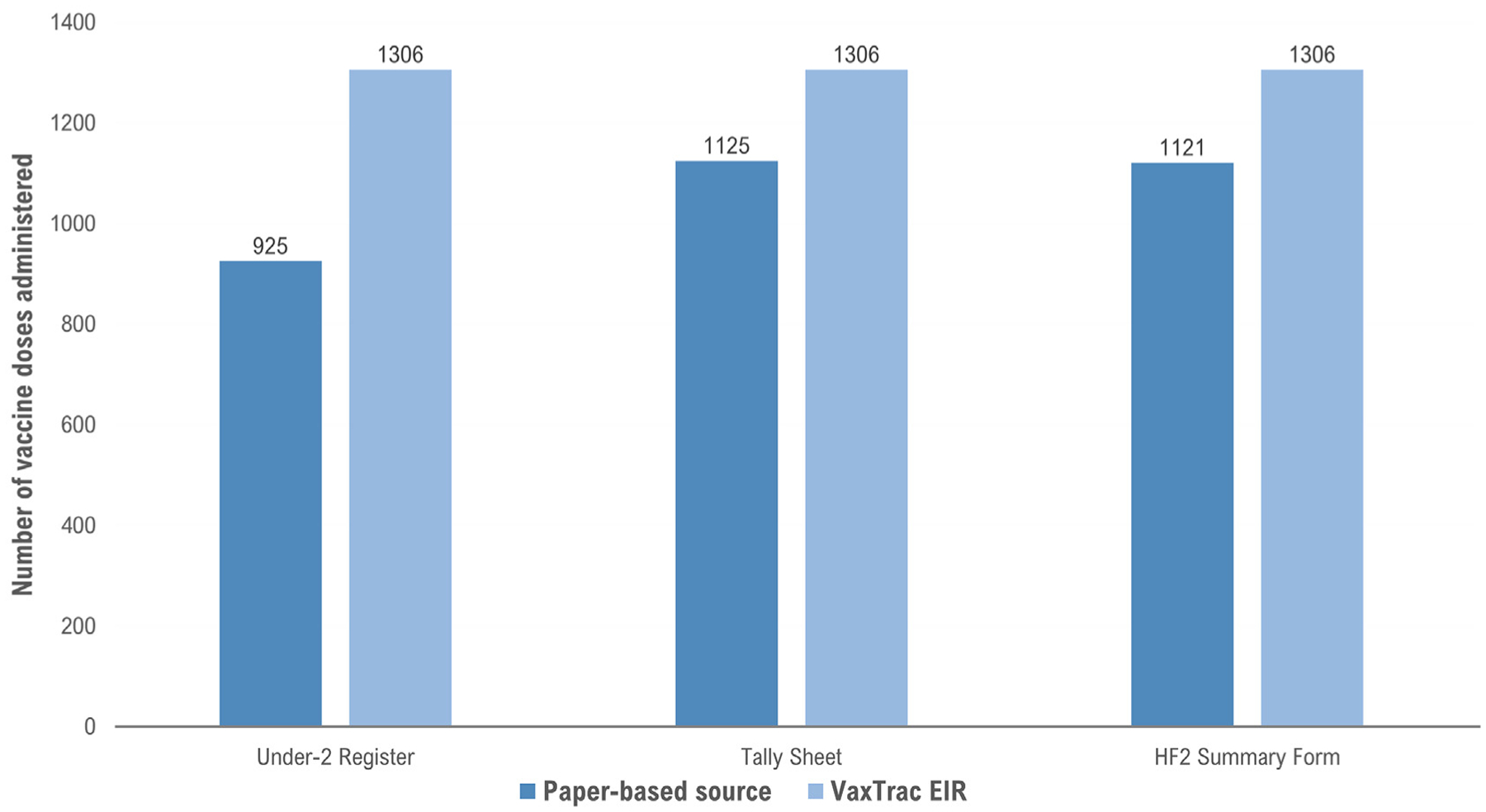
Ten out of 50 urban health facilities that implemented VaxTrac were purposively selected for inclusion in a rapid mixed-method assessment from November to December 2017. For a one-month period, records of six scheduled vaccine doses among children < 2 years old in VaxTrac were abstracted and compared to three paper-based records (register of under-two children, daily tally sheet, and monthly summary form). We used the under-two register as the reference gold standard for comparison purposes. We interviewed and observed 10 heath workers, one from each selected facility, who were using VaxTrac.
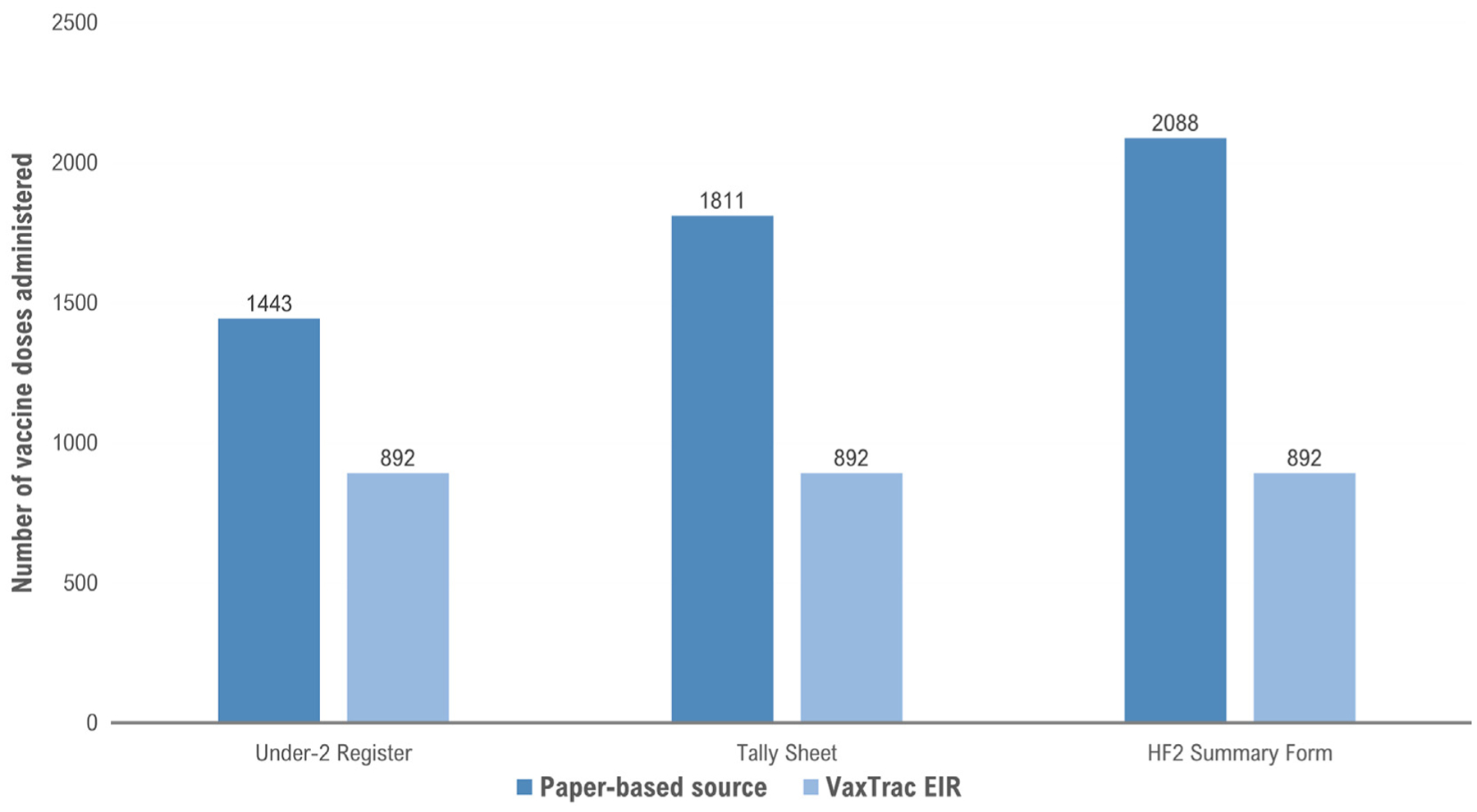
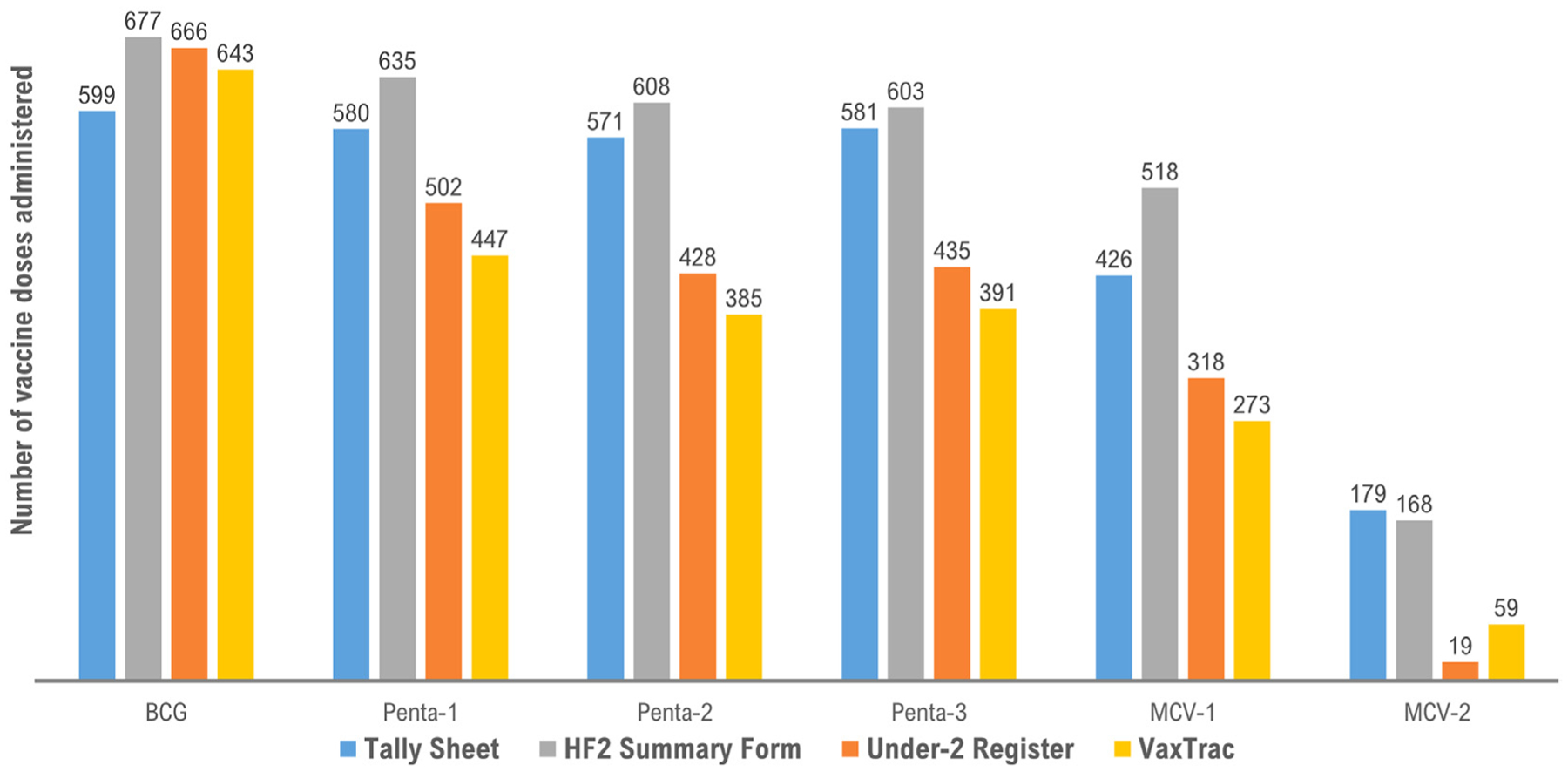
Overall, VaxTrac captured < 65% of the vaccine doses reported in the paper-based sources, but in the largest health facility VaxTrac captured the highest number of doses. Two additional notable patterns emerged: 1) the aggregated data sources reported higher doses administered compared to the under-two register and VaxTrac; 2) data sources that need real-time data capture during the vaccination session reported fewer doses administered compared to the monthly HF2 summary form. Health workers expressed that the EIR helped them to shorten the time to manage, summarize, and report vaccination records. Workflows for data entry in VaxTrac were inconsistent among facilities and rarely integrated into existing processes. Data sharing restrictions contributed to duplicate records.
Although VaxTrac helped to shorten the time to manage, summarize, and report vaccination records, data sharing restrictions coupled with inconsistent and inefficient workflows were major implementation challenges. Readiness-to-introduce and sustainability should be carefully considered before implementing an EIR.
2016 年,塞拉利昂卫生部和公共卫生署(MoHS)在一个城市地区试点了电子免疫登记系统(EIR)VaxTrac,以改善疫苗接种记录的管理和跟踪错过计划剂量的儿童。我们旨在记录经验教训,为 VaxTrac 和类似 EIR 的未来使用提供决策依据。
从 2017 年 11 月到 12 月,从实施 VaxTrac 的 50 个城市卫生机构中,有 10 个机构被有目的地选中参加快速混合方法评估。在一个月的时间里,从 VaxTrac 中抽取了 6 种计划疫苗剂量的儿童<2 岁的记录,并与三种基于纸张的记录(2 岁以下儿童登记册、每日计数表和每月汇总表)进行了比较。我们使用 2 岁以下登记册作为比较的参考黄金标准。我们采访和观察了 10 名卫生工作者,每个选定的机构都有一名,他们正在使用 VaxTrac。
总体而言,VaxTrac 记录的疫苗剂量<65%,但在最大的卫生机构中,VaxTrac 记录的剂量最高。还出现了两个值得注意的模式:1)汇总数据源报告的接种剂量高于 2 岁以下登记册和 VaxTrac;2)需要在接种期间实时数据录入的数据源报告的接种剂量低于每月 HF2 汇总表。卫生工作者表示,电子免疫登记系统帮助他们缩短了管理、汇总和报告疫苗接种记录的时间。VaxTrac 中的数据录入工作流程在各机构之间不一致,很少与现有流程整合。数据共享限制导致了重复记录。
尽管 VaxTrac 有助于缩短管理、汇总和报告疫苗接种记录的时间,但数据共享限制以及不一致和低效的工作流程是主要的实施挑战。在实施电子免疫登记系统之前,应仔细考虑准备情况和可持续性。