The University of Wisconsin School of Medicine & Public Health, Madison, WI.
Imaging Biomarkers and Computer-Aided Diagnosis Laboratory, Radiology and Imaging Sciences, National Institutes of Health Clinical Center, Bethesda, MD.
Lancet Digit Health. 2020 Apr;2(4):e192-e200. doi: 10.1016/S2589-7500(20)30025-X. Epub 2020 Mar 2.
Body CT scans are frequently performed for a wide variety of clinical indications, but potentially valuable biometric information typically goes unused. We investigated the prognostic ability of automated CT-based body composition biomarkers derived from previously-developed deep-learning and feature-based algorithms for predicting major cardiovascular events and overall survival in an adult screening cohort, compared with clinical parameters.
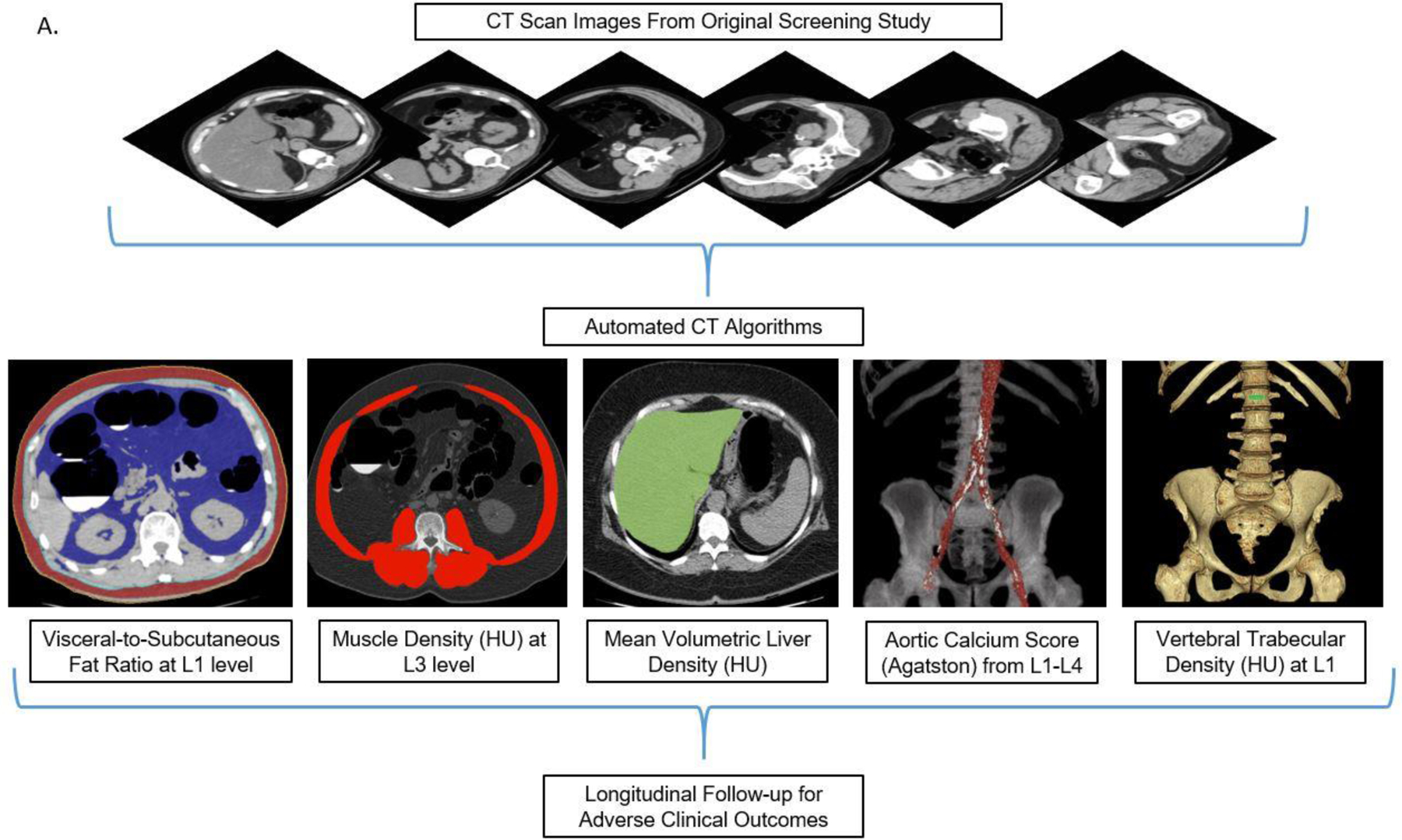
Mature and fully-automated CT-based algorithms with pre-defined metrics for quantifying aortic calcification, muscle density, visceral/subcutaneous fat, liver fat, and bone mineral density (BMD) were applied to a generally-healthy asymptomatic outpatient cohort of 9223 adults (mean age, 57.1 years; 5152 women) undergoing abdominal CT for routine colorectal cancer screening. Longitudinal clinical follow-up (median, 8.8 years; IQR, 5.1-11.6 years) documented subsequent major cardiovascular events or death in 19.7% (n=1831). Predictive ability of CT-based biomarkers was compared against the Framingham Risk Score (FRS) and body mass index (BMI).
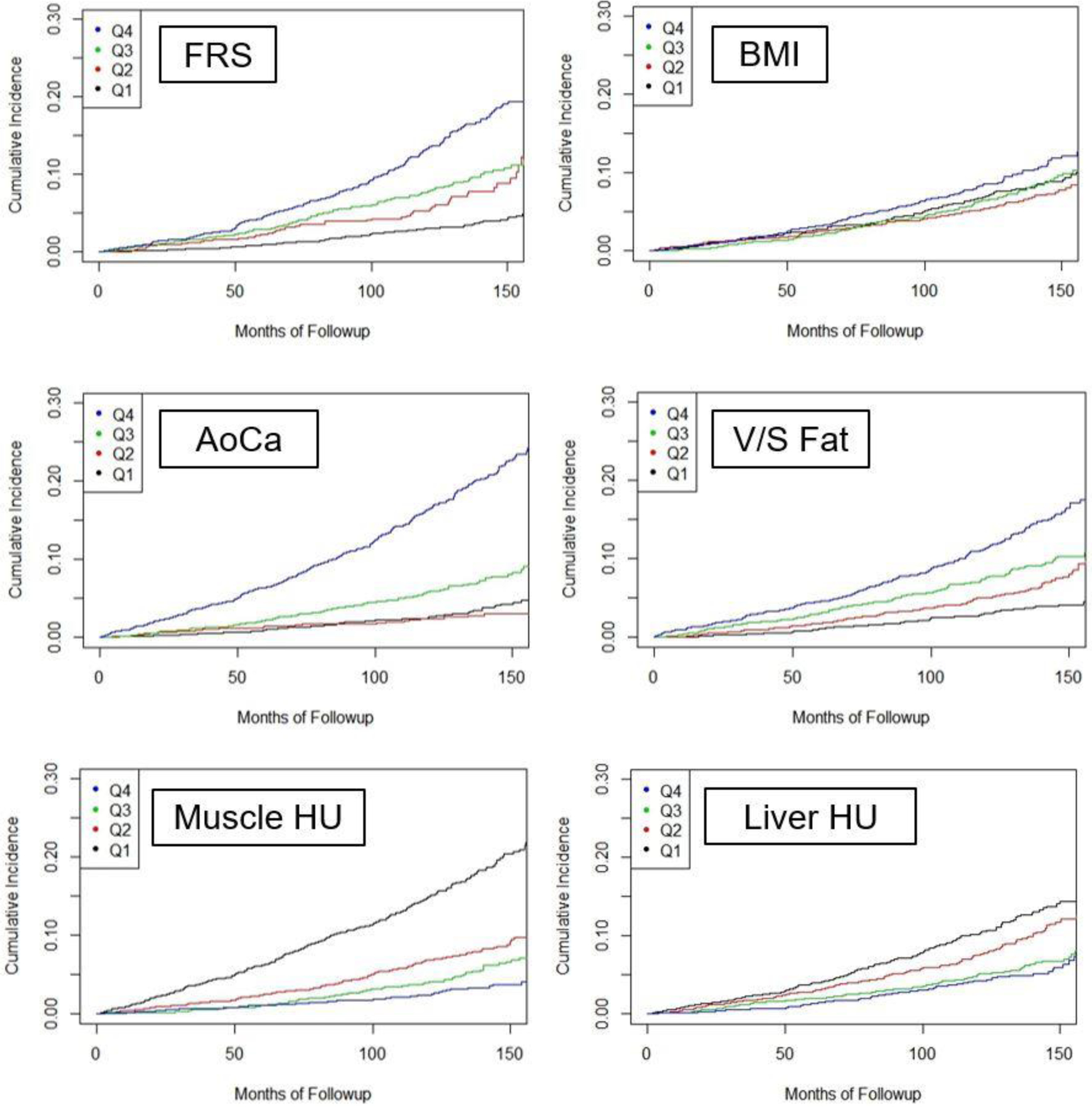
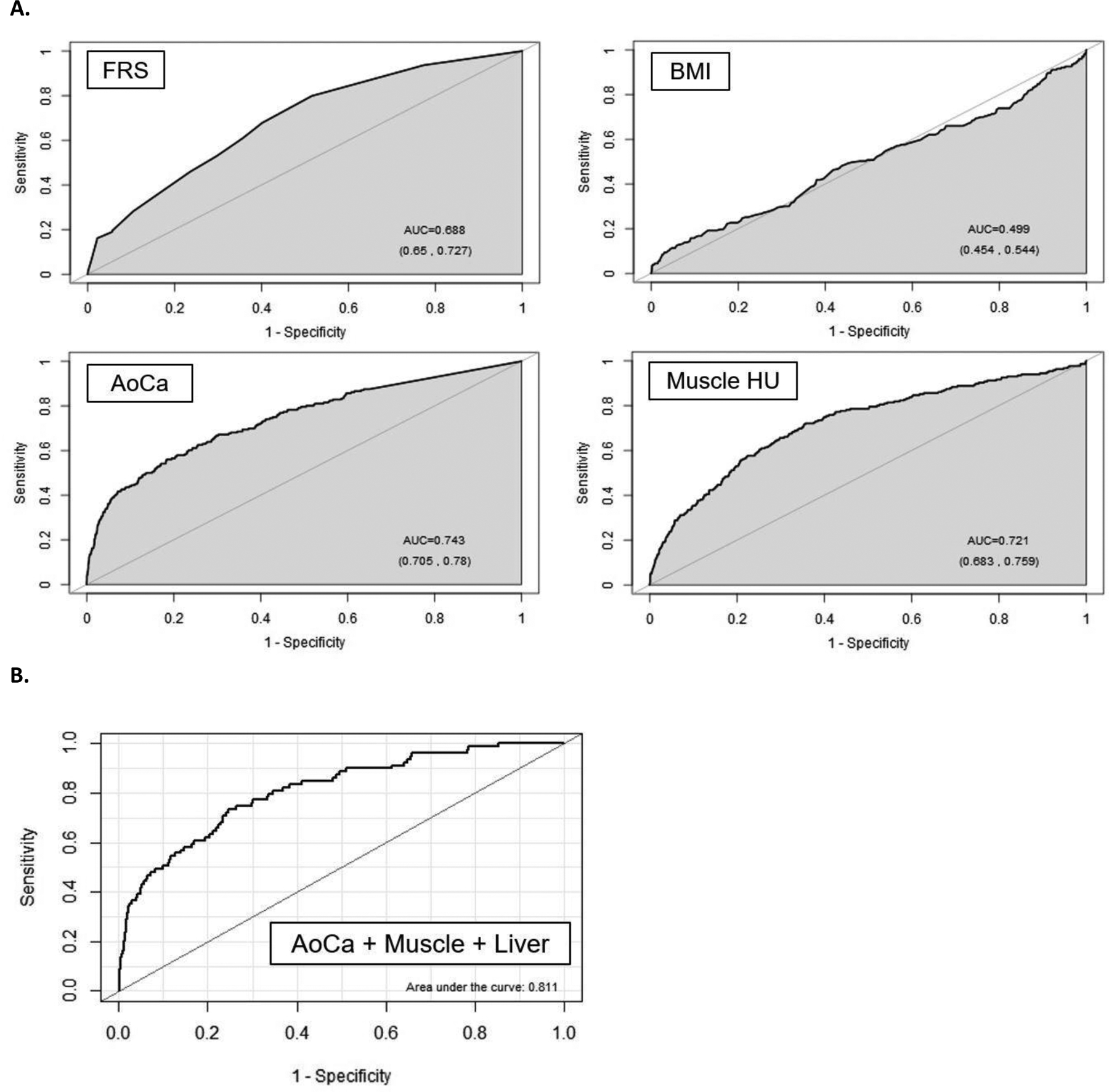
Significant differences were observed for all five automated CT-based body composition measures according to adverse events (p<0.001). Univariate 5-year AUROC (with 95% CI) for automated CT-based aortic calcification, muscle density, visceral/subcutaneous fat ratio, liver density, and vertebral density for predicting death were 0.743(0.705-0.780)/0.721(0.683-0.759)/0.661(0.625-0.697)/0.619 (0.582-0.656)/0.646(0.603-0.688), respectively, compared with 0.499(0.454-0.544) for BMI and 0.688(0.650-0.727) for FRS (p<0.05 for aortic calcification vs. FRS and BMI); all trends were similar for 2-year and 10-year ROC analyses. Univariate hazard ratios (with 95% CIs) for highest-risk quartile versus others for these same CT measures were 4.53(3.82-5.37) /3.58(3.02-4.23)/2.28(1.92-2.71)/1.82(1.52-2.17)/2.73(2.31-3.23), compared with 1.36(1.13-1.64) and 2.82(2.36-3.37) for BMI and FRS, respectively. Similar significant trends were observed for cardiovascular events. Multivariate combinations of CT biomarkers further improved prediction over clinical parameters (p<0.05 for AUROCs). For example, by combining aortic calcification, muscle density, and liver density, the 2-year AUROC for predicting overall survival was 0.811 (0.761-0.860).
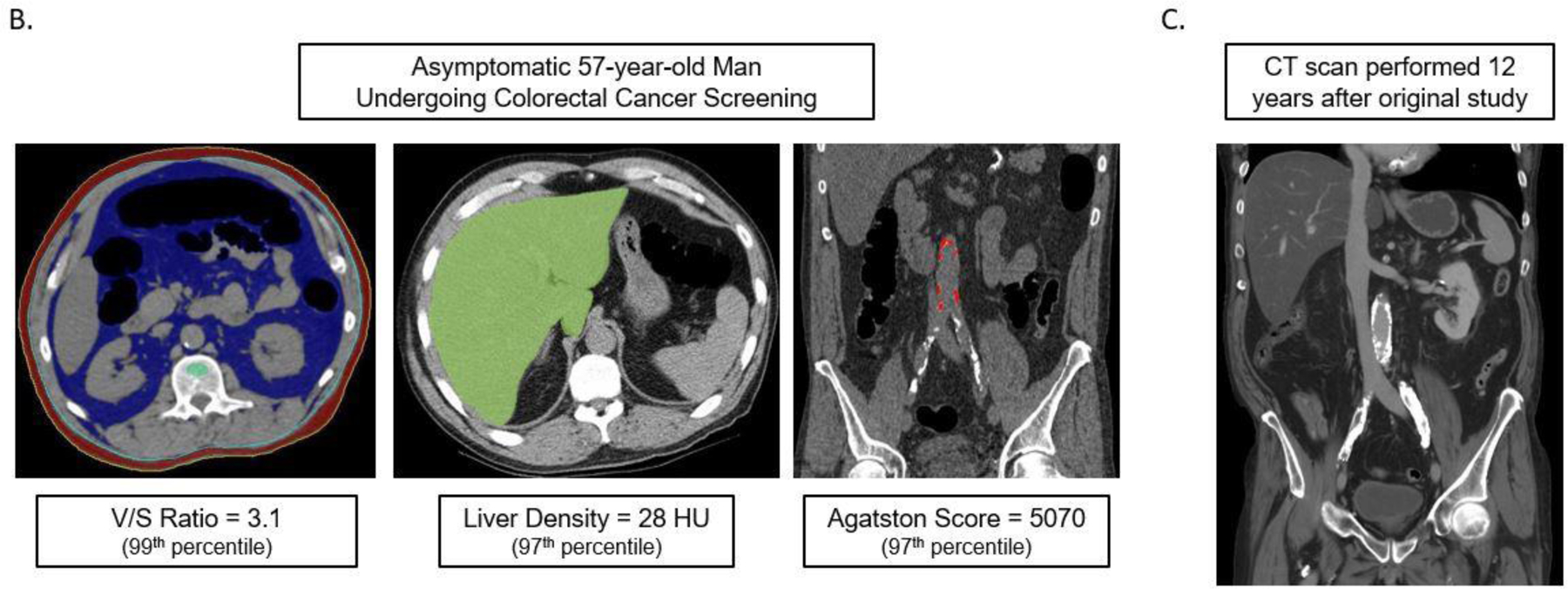
Fully-automated quantitative tissue biomarkers derived from CT scans can outperform established clinical parameters for pre-symptomatic risk stratification for future serious adverse events, and add opportunistic value to CT scans performed for other indications.
身体 CT 扫描常用于各种临床指征,但潜在的有价值的生物计量信息通常未被使用。我们研究了从以前开发的深度学习和基于特征的算法中得出的自动化 CT 身体成分生物标志物的预后能力,这些算法用于预测主要心血管事件和整体生存率,与临床参数进行比较。
成熟且完全自动化的 CT 算法,具有用于量化主动脉钙化、肌肉密度、内脏/皮下脂肪、肝脂肪和骨矿物质密度(BMD)的预定义指标,应用于接受腹部 CT 进行常规结直肠癌筛查的一般健康无症状门诊队列中的 9223 名成年人(平均年龄 57.1 岁;女性 5152 人)。纵向临床随访(中位数 8.8 年;IQR 5.1-11.6 年)记录了 19.7%(n=1831)的后续主要心血管事件或死亡。CT 生物标志物的预测能力与弗雷明汉风险评分(FRS)和体重指数(BMI)进行了比较。
根据不良事件,所有五种自动 CT 身体成分测量都有显著差异(p<0.001)。自动 CT 主动脉钙化、肌肉密度、内脏/皮下脂肪比、肝密度和椎体密度预测死亡的 5 年 AUROC(95%CI)分别为 0.743(0.705-0.780)/0.721(0.683-0.759)/0.661(0.625-0.697)/0.619(0.582-0.656)/0.646(0.603-0.688),而 BMI 的为 0.499(0.454-0.544),FRS 的为 0.688(0.650-0.727)(主动脉钙化与 FRS 和 BMI 相比,p<0.05);2 年和 10 年 ROC 分析的所有趋势均相似。对于这些相同的 CT 测量,最高风险四分位数与其他四分位数相比的单变量危险比(95%CI)分别为 4.53(3.82-5.37)/3.58(3.02-4.23)/2.28(1.92-2.71)/1.82(1.52-2.17)/2.73(2.31-3.23),而 BMI 和 FRS 分别为 1.36(1.13-1.64)和 2.82(2.36-3.37)。对于心血管事件也观察到类似的显著趋势。CT 生物标志物的多变量组合进一步提高了临床参数的预测(AUROCs 的 p<0.05)。例如,通过结合主动脉钙化、肌肉密度和肝密度,预测总生存率的 2 年 AUROC 为 0.811(0.761-0.860)。
从 CT 扫描中得出的全自动定量组织生物标志物可以优于既定的临床参数,用于预测未来严重不良事件的无症状风险分层,并为其他适应症进行的 CT 扫描提供机会性价值。