Harvard Medical School, Department of Global Health and Social Medicine, 641 Huntington Avenue, Boston, MA 02115, United States.
Brigham & Women's Hospital, Department of Obstetrics, Gynecology, and Reproductive Biology, 75 Francis Street, Boston, MA 02115, United States; Harvard Medical School, 25 Shattuck Street, Boston, MA 02115, United States.
Contraception. 2020 Dec;102(6):385-391. doi: 10.1016/j.contraception.2020.08.017. Epub 2020 Sep 6.
To quantify the number of medically unnecessary clinical visits and in-clinic contacts monthly caused by US abortion regulations.
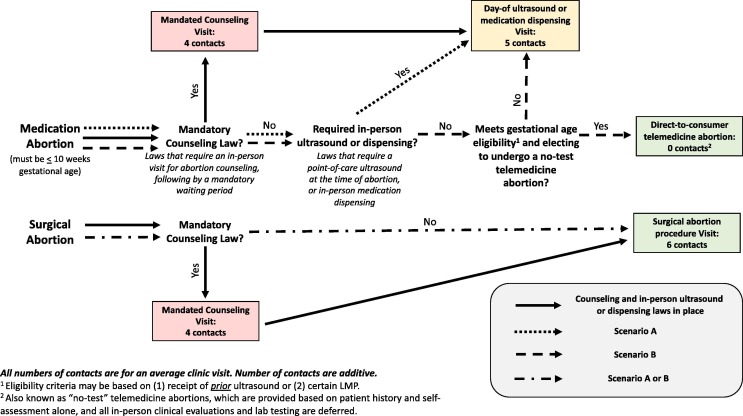
We estimated the number of clinical visits and clinical contacts (any worker a patient may come into physical contact with during their visit) under the current policy landscape, compared to the number of visits and contacts if the following regulations were repealed: (1) State mandatory in-person counseling visit laws that necessitate two visits for abortion, (2) State mandatory-ultrasound laws, (3) State mandates requiring the prescribing clinician be present during mifepristone administration, (4) Federal Food and Drug Administration Risk Evaluation and Mitigation Strategy for mifepristone. If these laws were repealed, "no-test" telemedicine abortion would be possible for some patients. We modeled the number of visits averted if a minimum of 15 percent or a maximum of 70 percent of medication abortion patients had a "no-test" telemedicine abortion.
We estimate that 12,742 in-person clinic visits (50,978 clinical contacts) would be averted each month if counseling visit laws alone were repealed, and 31,132 visits (142,910 clinical contacts) would be averted if all four policies were repealed and 70 percent of medication abortion patients received no-test telemedicine abortions. Over 2 million clinical contacts could be averted over the projected 18-month COVID-19 pandemic.
Medically unnecessary abortion regulations result in a large number of excess clinical visits and contacts.
Repeal of medically unnecessary state and federal abortion restrictions in the United States would allow for evidence-based telemedicine abortion care, thereby lowering risk of SARS-CoV-2 transmission.
量化因美国堕胎法规而每月导致的不必要医疗就诊次数和临床接触次数。
我们估算了在当前政策环境下的就诊次数和临床接触次数(患者在就诊期间可能与任何工作人员进行身体接触),并与以下法规被废除的情况下的就诊次数和接触次数进行了比较:(1)要求堕胎必须进行两次现场咨询的州强制性规定,(2)州强制性超声法规,(3)要求在米非司酮给药期间主治医生在场的规定,(4)联邦食品和药物管理局对米非司酮的风险评估和缓解策略。如果这些法规被废除,一些患者可以进行“无检测”远程医疗堕胎。我们对如果有 15%至 70%的药物流产患者进行“无检测”远程医疗堕胎,可避免的就诊次数进行了建模。
我们估计,如果仅废除咨询访问法规,每月将避免 12742 次现场诊所就诊(50978 次临床接触),如果所有四项政策都被废除,并且 70%的药物流产患者接受“无检测”远程医疗堕胎,则可避免 31132 次就诊(142910 次临床接触)。在预计的 18 个月的 COVID-19 大流行期间,可避免超过 200 万次临床接触。
不必要的堕胎法规导致了大量不必要的医疗就诊次数和接触次数。
在美国废除不必要的州和联邦堕胎限制将允许基于证据的远程医疗堕胎护理,从而降低 SARS-CoV-2 传播的风险。