Department of Women's, Gender & Sexuality Studies, University of Cincinnati, Cincinnati, OH, United States.
Division of Epidemiology, College of Public Health, Ohio State University, Columbus, OH, United States.
Contraception. 2021 Jul;104(1):111-116. doi: 10.1016/j.contraception.2021.04.020. Epub 2021 Apr 27.
We aimed to characterize the combined impact of federal, state, and institutional policies on barriers to expanding medication and telemedicine abortion care delivery during the COVID-19 pandemic in the abortion-restrictive states of Ohio, Kentucky, and West Virginia.
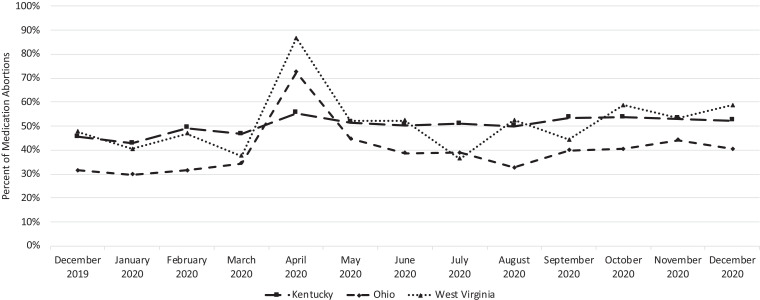
We analyzed 4 state policies, 2 COVID-related state executive orders, and clinic-level survey data on medication abortion provision from fourteen abortion facilities in Ohio, Kentucky, and West Virginia from December 2019 to December 2020. We calculated the percent of medication abortions provided at these facilities during the study period by state, to assess changes in medication abortion use during the pandemic.
We ascertained that COVID-19-executive orders in Ohio and West Virginia that limited procedural abortion in Spring 2020 coincided with an increase in the overall number and proportion of medication abortions in this region, peaking at 1613 medication abortions (70%) in April 2020. Ohio and West Virginia, which had executive orders limiting procedural abortion, saw relatively greater increases in April compared to Kentucky. Despite temporary lifting of the mifepristone REMS, prepandemic regulations banning telemedicine abortion in Kentucky and West Virginia and requiring in-person clinic visits for medication abortion distribution in Ohio limited clinics' ability to adapt to offer medication abortion by mail.
Our findings illustrate how restrictive medication and telemedicine abortion policies in Ohio, Kentucky, and West Virginia created additional obstacles for patients seeking medication abortion during the pandemic. Permanently lifting federal regulations on in-clinic distribution of mifepristone would only advantage abortion seekers in states without restrictive telehealth and medication abortion policies. State policies that limit access to comprehensive abortion services should be central in larger efforts toward dismantling barriers that impinge upon reproductive autonomy.
We find that abolishing the REMS on mifepristone would not be enough to expand access to patients in abortion-restrictive states with telemedicine and medication abortion laws. While the REMS is a barrier, it represents one of several hindrances to the expansion of telemedicine abortion distribution across the United States.
我们旨在描述联邦、州和机构政策对俄亥俄州、肯塔基州和西弗吉尼亚州在 COVID-19 大流行期间扩大药物和远程医疗堕胎护理服务的障碍的综合影响。
我们分析了俄亥俄州、肯塔基州和西弗吉尼亚州的 4 项州政策、2 项与 COVID 相关的州行政命令以及来自俄亥俄州、肯塔基州和西弗吉尼亚州的 14 家堕胎机构在 2019 年 12 月至 2020 年 12 月期间提供药物堕胎的诊所水平调查数据。我们按州计算了研究期间这些机构提供的药物堕胎百分比,以评估大流行期间药物堕胎使用的变化。
我们发现,俄亥俄州和西弗吉尼亚州的 COVID-19 行政命令限制了 2020 年春季的程序堕胎,这与该地区药物堕胎总数和比例的增加同时发生,2020 年 4 月达到 1613 例药物堕胎(70%)的峰值。俄亥俄州和西弗吉尼亚州有行政命令限制程序堕胎,与肯塔基州相比,4 月份的增幅相对较大。尽管米非司酮的 REMS 暂时被取消,但肯塔基州和西弗吉尼亚州禁止远程医疗堕胎的前期法规以及俄亥俄州要求亲自到诊所就诊以分发药物堕胎的规定限制了诊所通过邮件提供药物堕胎的能力。
我们的研究结果表明,俄亥俄州、肯塔基州和西弗吉尼亚州对药物和远程医疗堕胎的限制政策如何为大流行期间寻求药物堕胎的患者增加了额外的障碍。永久取消联邦对米非司酮在诊所分发的规定只会使没有限制远程医疗和药物堕胎政策的州的堕胎寻求者受益。限制全面堕胎服务机会的州政策应成为消除影响生殖自主权的障碍的更大努力的核心。
我们发现,取消米非司酮的 REMS 不足以扩大在具有远程医疗和药物堕胎法的堕胎限制州的患者获得药物的机会。虽然 REMS 是一个障碍,但它代表了在美国扩大远程医疗堕胎服务的几个障碍之一。