Department of Pediatrics, Renmin Hospital of Wuhan University, Wuhan, China.
Department of Biology and Genetics, College of Life Sciences and Health, Wuhan University of Science and Technology, Wuhan, China.
Front Immunol. 2020 Aug 28;11:2075. doi: 10.3389/fimmu.2020.02075. eCollection 2020.
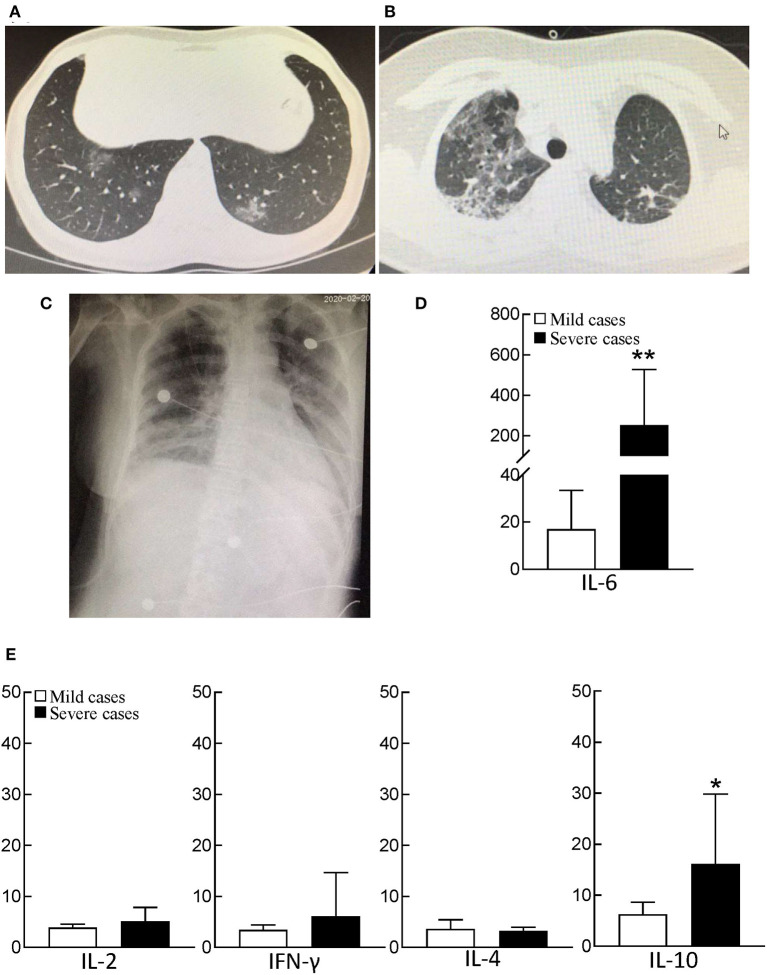
To explore the metabolic changes and immune profiles in patients with COVID-19, we analyzed the data of patients with mild and severe COVID-19 as well as young children with COVID-19. Of the leukocytes, 47% (IQR, 33-59) were lymphocytes [2.5 × 10/L (IQR, 2.2-3.3)], and monocytes were 0.51 × 10/L (IQR, 0.45-0.57) in young children with COVID-19. In 32 mild COVID-19 patients, circulating monocytes were 0.45 × 10/L (IQR, 0.36-0.64). Twenty-one severe patients had low PO [57 mmHg (IQR, 50-73)] and SO [90% (IQR, 86-93)] and high lactate dehydrogenase [580 U/L (IQR, 447-696)], cardiac troponin I [0.07 ng/mL (IQR, 0.02-0.30)], and pro-BNP [498 pg/mL (IQR, 241-1,726)]. Serum D-dimer and FDP were 9.89 mg/L (IQR, 3.62-22.85) and 32.7 mg/L (IQR, 12.8-81.9), and a large number of RBC (46/μL (IQR, 4-242) was presented in urine, a cue of disseminated intravascular coagulation (DIC) in severe patients. Three patients had comorbidity with diabetes, and 18 patients without diabetes also presented high blood glucose [7.4 mmol/L (IQR, 5.9-10.1)]. Fifteen of 21 (71%) severe cases had urine glucose +, and nine of 21 (43%) had urine ketone body +. The increased glucose was partially caused by reduced glucose consumption of cells. Severe cases had extraordinarily low serum uric acid [176 μmol/L (IQR, 131-256)]. In the late stage of COVID-19, severe cases had extremely low CD4 T cells and CD8 T cells, but unusually high neutrophils [6.5 × 10/L (IQR, 4.8-9.6)], procalcitonin [0.27 ng/mL (IQR, 0.14-1.94)], C-reactive protein [66 mg/L (IQR, 25-114)] and an extremely high level of interleukin-6. Four of 21 (19%) severe cases had co-infection with fungi, and two of 21 (9%) severe cases had bacterial infection. Our findings suggest that, severe cases had acute respiratory distress syndrome (ARDS) I-III, and metabolic disorders of glucose, lipid, uric acid, etc., even multiple organ dysfunction (MODS) and DIC. Increased neutrophils and severe inflammatory responses were involved in ARDS, MODS, and DIC. With the dramatical decrease of T-lymphocytes, severe cases were susceptible to co-infect with bacteria and fungi in the late stage of COVID-19. In young children, extremely high lymphocytes and monocytes might be associated with the low morbidity of COVID-19. The significantly increased monocytes might play an important role in the recovery of patients with mild COVID-19.
为了探究 COVID-19 患者的代谢变化和免疫特征,我们分析了轻症和重症 COVID-19 患者以及感染 COVID-19 的幼儿的数据。在白细胞中,淋巴细胞占 47%(IQR,33-59)[2.5×10/L(IQR,2.2-3.3)],幼儿的单核细胞为 0.51×10/L(IQR,0.45-0.57)。在 32 例轻症 COVID-19 患者中,循环单核细胞为 0.45×10/L(IQR,0.36-0.64)。21 例重症患者有低 PO[57mmHg(IQR,50-73)]和 SO[90%(IQR,86-93)],以及高乳酸脱氢酶[580U/L(IQR,447-696)]、心肌肌钙蛋白 I[0.07ng/mL(IQR,0.02-0.30)]和 pro-BNP[498pg/mL(IQR,241-1726)]。血清 D-二聚体和 FDP 分别为 9.89mg/L(IQR,3.62-22.85)和 32.7mg/L(IQR,12.8-81.9),尿液中大量出现 RBC(46/μL(IQR,4-242),提示重症患者存在弥散性血管内凝血(DIC)。3 例患者合并糖尿病,18 例无糖尿病患者也出现高血糖[7.4mmol/L(IQR,5.9-10.1)]。21 例重症患者中,15 例(71%)有尿葡萄糖+,21 例(43%)有尿酮体+。升高的血糖部分是由于细胞葡萄糖消耗减少所致。重症患者血清尿酸极低[176μmol/L(IQR,131-256)]。在 COVID-19 晚期,重症患者的 CD4+T 细胞和 CD8+T 细胞极低,但中性粒细胞异常升高[6.5×10/L(IQR,4.8-9.6)]、降钙素原[0.27ng/mL(IQR,0.14-1.94)]、C 反应蛋白[66mg/L(IQR,25-114)]和白细胞介素-6 水平极高。21 例重症患者中,4 例(19%)合并真菌感染,21 例重症患者中,2 例(9%)合并细菌感染。我们的研究结果表明,重症患者存在急性呼吸窘迫综合征(ARDS)I-III 级,以及葡萄糖、脂质、尿酸等代谢紊乱,甚至多器官功能障碍(MODS)和弥散性血管内凝血(DIC)。中性粒细胞增加和严重的炎症反应参与了 ARDS、MODS 和 DIC。随着 T 淋巴细胞的急剧减少,重症患者在 COVID-19 晚期易合并细菌和真菌感染。在幼儿中,极高的淋巴细胞和单核细胞可能与 COVID-19 的低发病率有关。显著增加的单核细胞可能在轻症 COVID-19 患者的康复中发挥重要作用。