Division of Cardiology, Department of Medicine, University of Michigan, Frankel Cardiovascular Center, 1500 East Medical Center Drive, Ann Arbor, MI 48109, USA
Department of Internal Medicine, Hackensack Meridian School of Medicine at Seton Hall, Nutley, NJ, USA.
BMJ. 2020 Sep 30;371:m3513. doi: 10.1136/bmj.m3513.
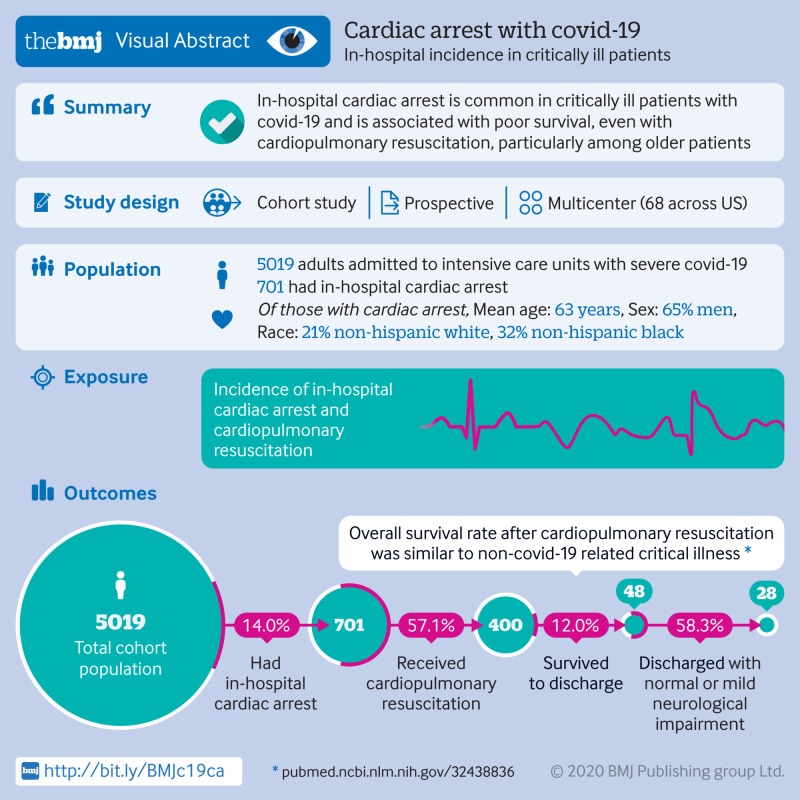
To estimate the incidence, risk factors, and outcomes associated with in-hospital cardiac arrest and cardiopulmonary resuscitation in critically ill adults with coronavirus disease 2019 (covid-19).
Multicenter cohort study.
Intensive care units at 68 geographically diverse hospitals across the United States.
Critically ill adults (age ≥18 years) with laboratory confirmed covid-19.
In-hospital cardiac arrest within 14 days of admission to an intensive care unit and in-hospital mortality.
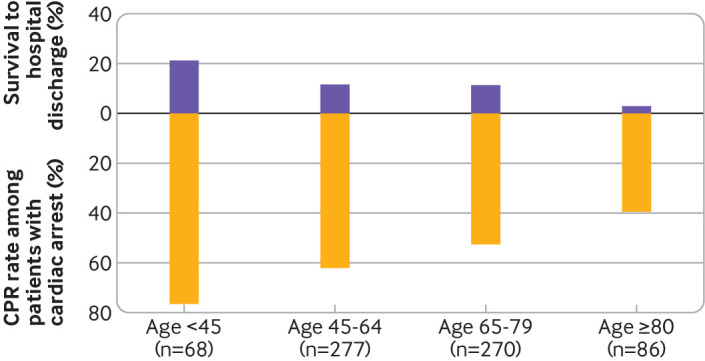
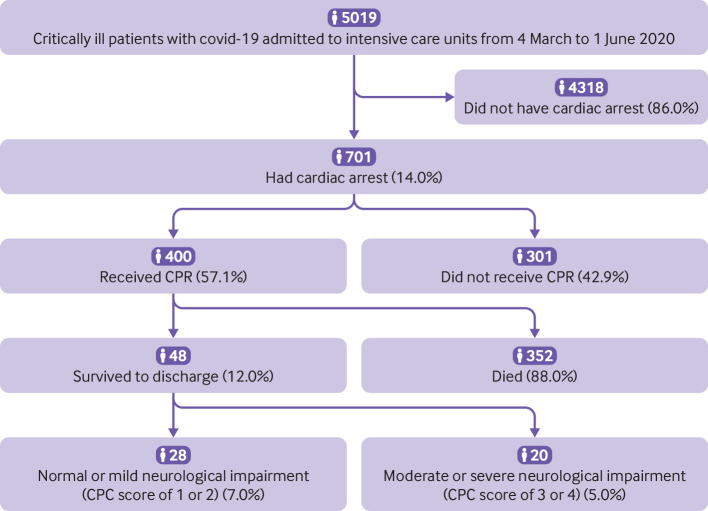
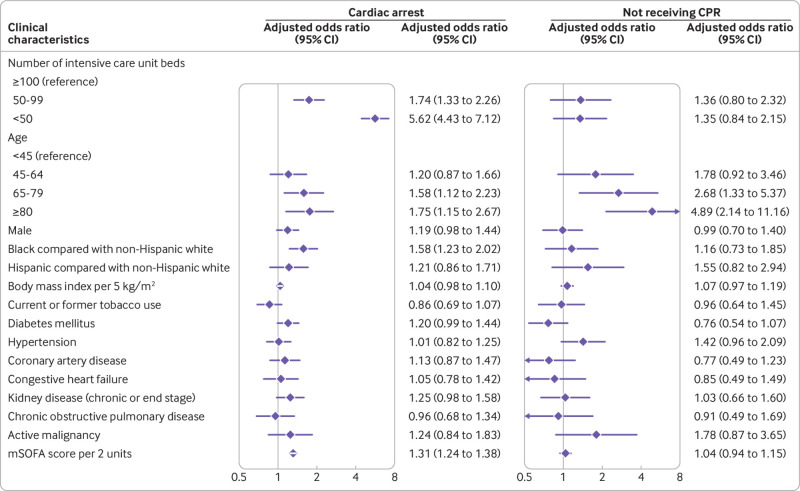
Among 5019 critically ill patients with covid-19, 14.0% (701/5019) had in-hospital cardiac arrest, 57.1% (400/701) of whom received cardiopulmonary resuscitation. Patients who had in-hospital cardiac arrest were older (mean age 63 (standard deviation 14) 60 (15) years), had more comorbidities, and were more likely to be admitted to a hospital with a smaller number of intensive care unit beds compared with those who did not have in-hospital cardiac arrest. Patients who received cardiopulmonary resuscitation were younger than those who did not (mean age 61 (standard deviation 14) 67 (14) years). The most common rhythms at the time of cardiopulmonary resuscitation were pulseless electrical activity (49.8%, 199/400) and asystole (23.8%, 95/400). 48 of the 400 patients (12.0%) who received cardiopulmonary resuscitation survived to hospital discharge, and only 7.0% (28/400) survived to hospital discharge with normal or mildly impaired neurological status. Survival to hospital discharge differed by age, with 21.2% (11/52) of patients younger than 45 years surviving compared with 2.9% (1/34) of those aged 80 or older.
Cardiac arrest is common in critically ill patients with covid-19 and is associated with poor survival, particularly among older patients.
评估与 2019 年冠状病毒病(COVID-19)相关的危重症成年患者院内心搏骤停和心肺复苏的发生率、危险因素和结局。
多中心队列研究。
美国 68 家地理位置不同的医院的重症监护病房。
患有经实验室证实的 COVID-19 的危重症成年患者(年龄≥18 岁)。
入院后 14 天内院内心搏骤停和院内死亡率。
在 5019 例患有 COVID-19 的危重症患者中,有 14.0%(701/5019)发生院内心搏骤停,其中 57.1%(400/701)接受了心肺复苏。发生院内心搏骤停的患者年龄较大(平均年龄 63(标准差 14) 60(15)岁),合并症更多,并且更有可能入住重症监护床位较少的医院。与未发生院内心搏骤停的患者相比,接受心肺复苏的患者更年轻(平均年龄 61(标准差 14) 67(14)岁)。心肺复苏时最常见的节律是无脉电活动(49.8%,199/400)和心搏停止(23.8%,95/400)。在接受心肺复苏的 400 名患者中,有 48 名(12.0%)存活至出院,仅有 7.0%(28/400)存活至出院且神经功能正常或轻度受损。出院存活率因年龄而异,年龄小于 45 岁的患者中有 21.2%(11/52)存活,而年龄 80 岁或以上的患者中仅有 2.9%(1/34)存活。
心搏骤停在 COVID-19 危重症患者中很常见,与预后不良相关,尤其是在老年患者中。