Sun Le-Jia, Guan Ai, Xu Wei-Yu, Liu Mei-Xi, Yin Huan-Huan, Jin Bao, Xu Gang, Xie Fei-Hu, Xu Hai-Feng, Du Shun-Da, Xu Yi-Yao, Zhao Hai-Tao, Lu Xin, Sang Xin-Ting, Yang Hua-Yu, Mao Yi-Lei
Department of Liver Surgery, Peking Union Medical College Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing 100730, China.
Department of Clinical Medicine, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing 100730, China.
World J Gastrointest Oncol. 2020 Sep 15;12(9):1014-1030. doi: 10.4251/wjgo.v12.i9.1014.
Gallbladder carcinoma (GBC) carries a poor prognosis and requires a prediction method. Gamma-glutamyl transferase-to-platelet ratio (GPR) is a recently reported cancer prognostic factor. Although the mechanism for the relationship between GPR and poor cancer prognosis remains unclear, studies have demonstrated the clinical effect of both gamma-glutamyl transferase and platelet count on GBC and related gallbladder diseases.
To assess the prognostic value of GPR and to design a prognostic nomogram for GBC.
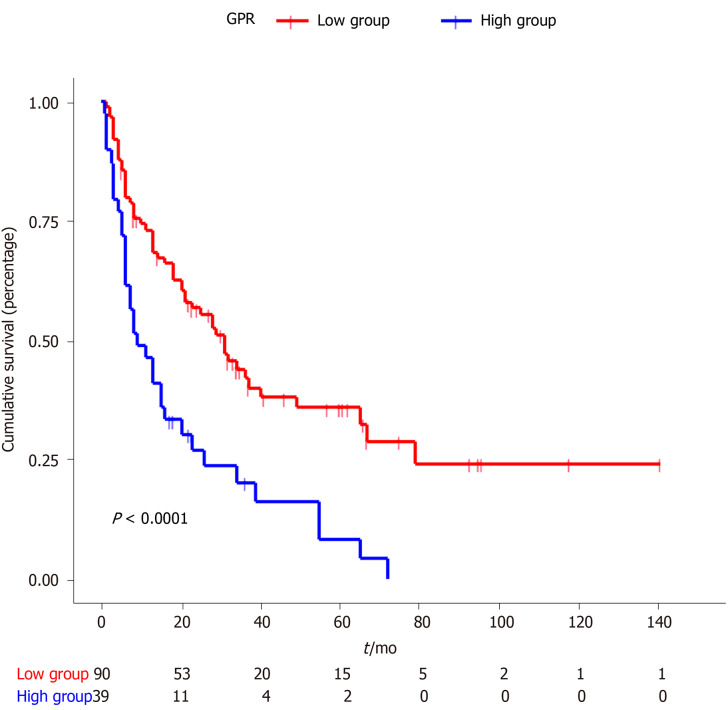
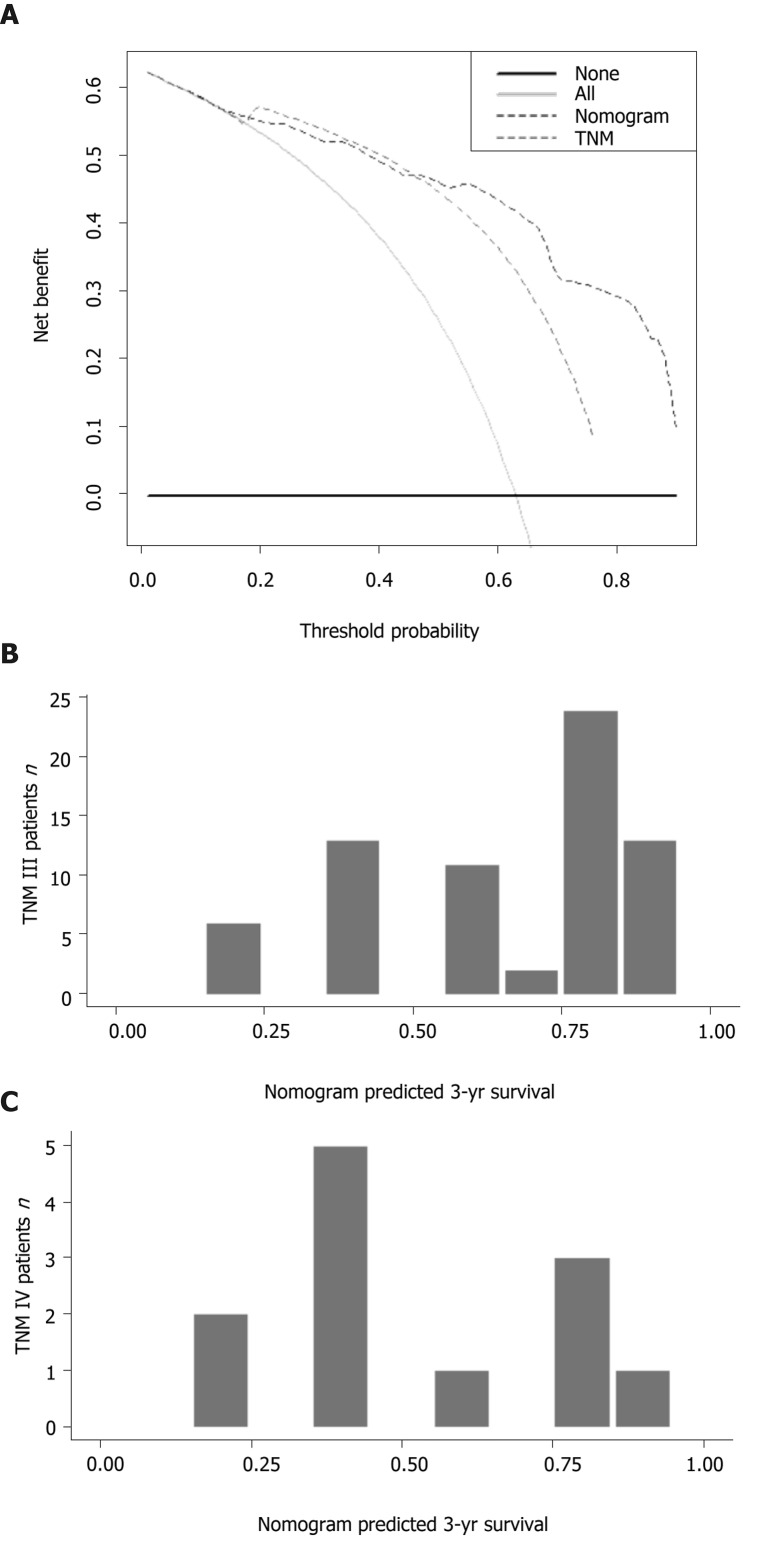
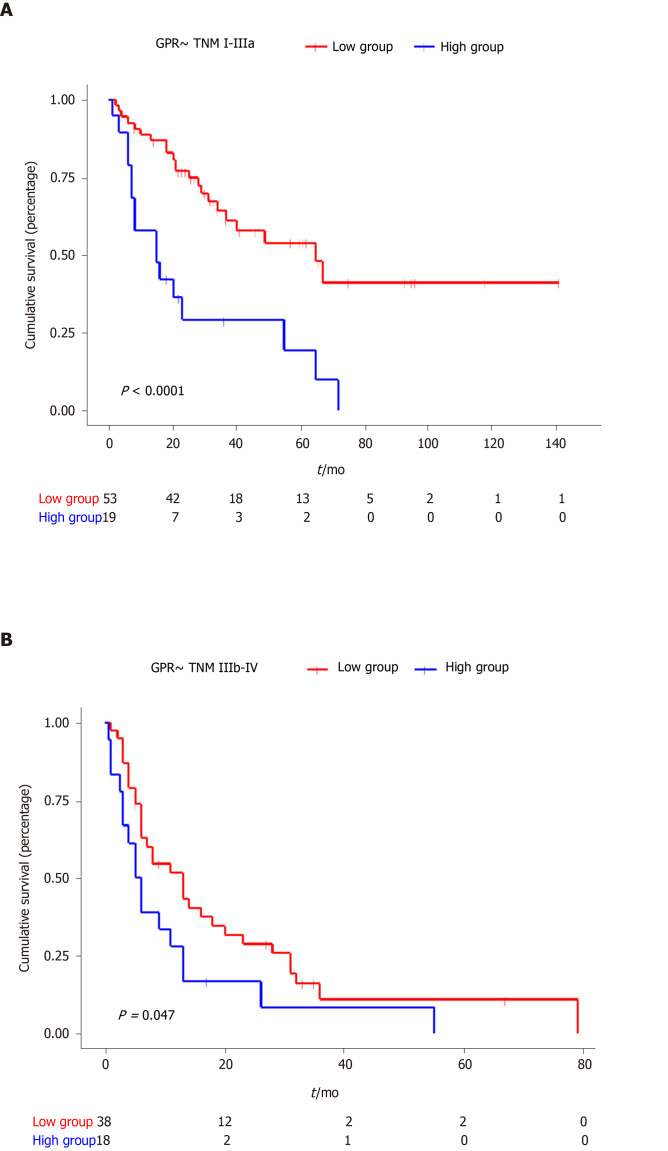
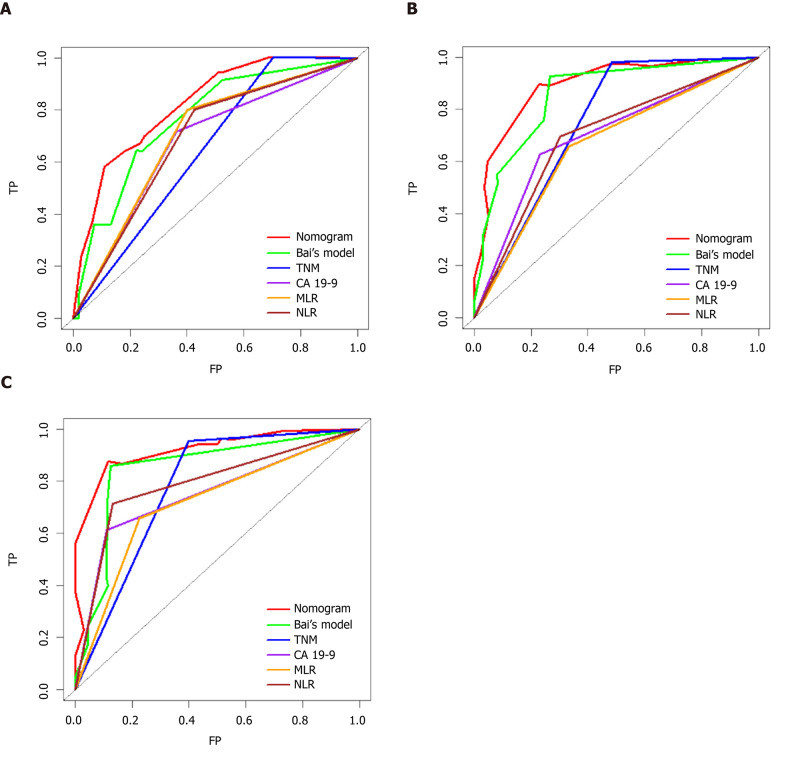
The analysis involved 130 GBC patients who underwent surgery at Peking Union Medical College Hospital from December 2003 to April 2017. The patients were stratified into a high- or low-GPR group. The predictive ability of GPR was evaluated by Kaplan-Meier analysis and a Cox regression model. We developed a nomogram based on GPR, which we verified using calibration curves. The nomogram and other prognosis prediction models were compared using time-dependent receiver operating characteristic curves and the concordance index.
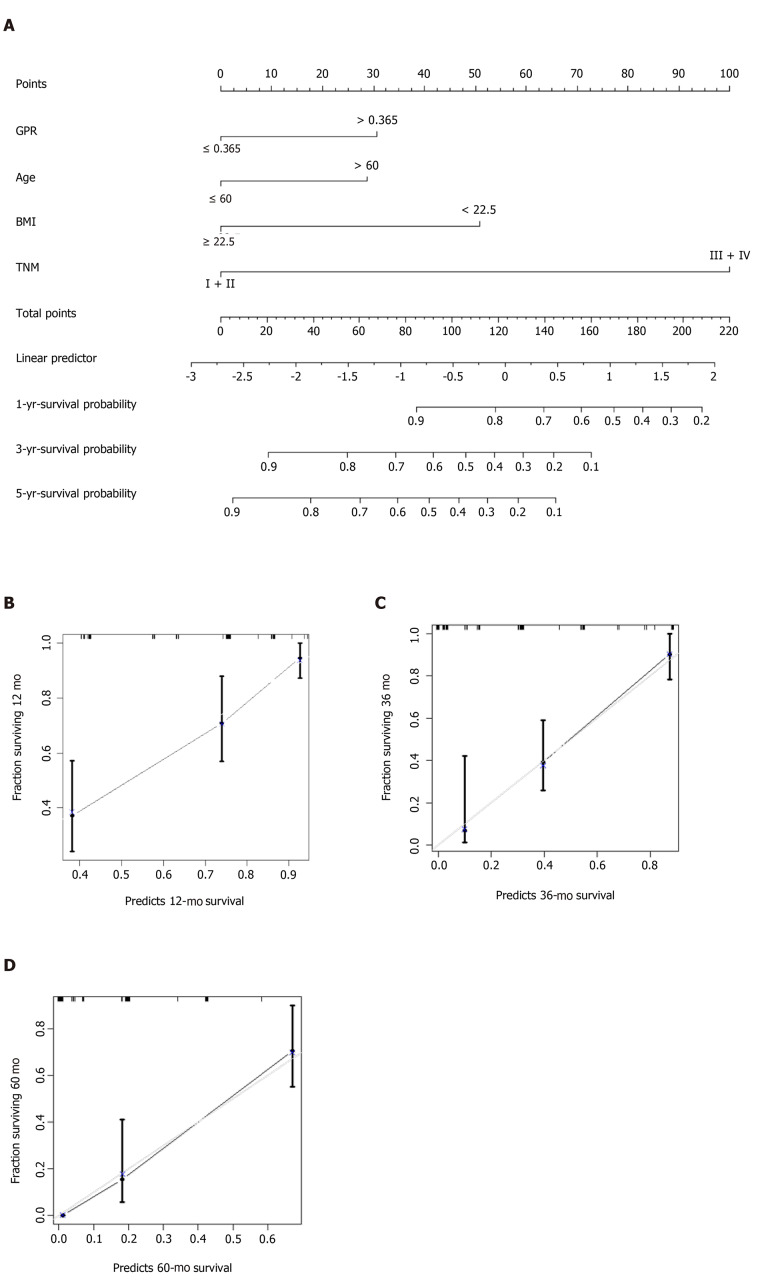
Patients in the high-GPR group had a higher risk of jaundice, were older, and had higher carbohydrate antigen 19-9 levels and worse postoperative outcomes. Univariate analysis revealed that GPR, age, body mass index, tumor-node-metastasis (TNM) stage, jaundice, cancer cell differentiation degree, and carcinoembryonic antigen and carbohydrate antigen 19-9 levels were related to overall survival (OS). Multivariate analysis confirmed that GPR, body mass index, age, and TNM stage were independent predictors of poor OS. Calibration curves were highly consistent with actual observations. Comparisons of time-dependent receiver operating characteristic curves and the concordance index showed advantages for the nomogram over TNM staging.
GPR is an independent predictor of GBC prognosis, and nomogram-integrated GPR is a promising predictive model for OS in GBC.
胆囊癌(GBC)预后较差,需要一种预测方法。γ-谷氨酰转移酶与血小板比值(GPR)是最近报道的癌症预后因素。尽管GPR与癌症预后不良之间关系的机制尚不清楚,但研究已经证明γ-谷氨酰转移酶和血小板计数对GBC及相关胆囊疾病的临床影响。
评估GPR的预后价值,并为GBC设计一种预后列线图。
分析2003年12月至2017年4月在北京协和医院接受手术的130例GBC患者。将患者分为高GPR组或低GPR组。通过Kaplan-Meier分析和Cox回归模型评估GPR的预测能力。我们基于GPR开发了一种列线图,并使用校准曲线进行验证。使用时间依赖性受试者工作特征曲线和一致性指数比较列线图和其他预后预测模型。
高GPR组患者黄疸风险更高、年龄更大、糖类抗原19-9水平更高且术后结果更差。单因素分析显示,GPR、年龄、体重指数、肿瘤-淋巴结-转移(TNM)分期、黄疸、癌细胞分化程度以及癌胚抗原和糖类抗原19-9水平与总生存期(OS)相关。多因素分析证实,GPR、体重指数、年龄和TNM分期是OS不良的独立预测因素。校准曲线与实际观察结果高度一致。时间依赖性受试者工作特征曲线和一致性指数的比较显示列线图优于TNM分期。
GPR是GBC预后的独立预测因素,整合GPR的列线图是GBC中一种有前景的OS预测模型。