Department of Cardiology, Sahlgrenska University Hospital, Sweden.
Department of Cardiology, Clinical Sciences, Lund University, Sweden.
Eur Heart J Acute Cardiovasc Care. 2020 Jun;9(4):323-332. doi: 10.1177/2048872620908032.
The purpose of this observational study was to evaluate the effects of radial artery access versus femoral artery access on the risk of 30-day mortality, inhospital bleeding and cardiogenic shock in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention.
We used data from the SWEDEHEART registry and included all patients who were treated with primary percutaneous coronary intervention in Sweden between 2005 and 2016. We compared patients who had percutaneous coronary intervention by radial access versus femoral access with regard to the primary endpoint of all-cause death within 30 days, using a multilevel propensity score adjusted logistic regression which included hospital as a random effect.
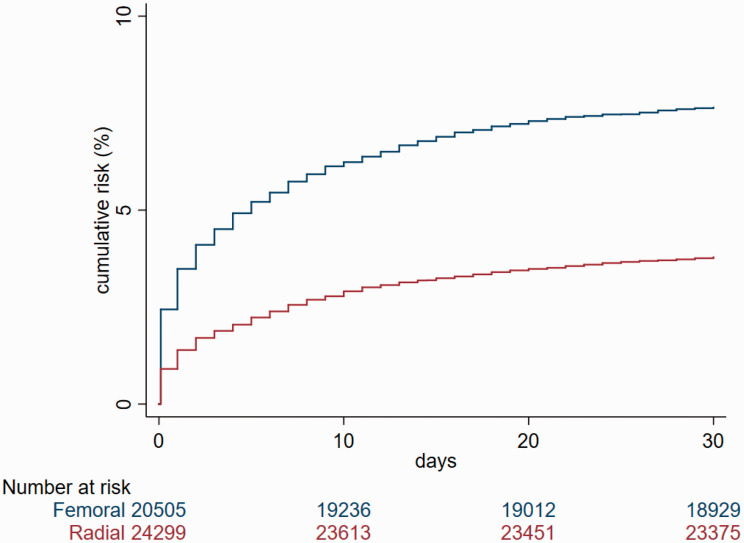
During the study period, 44,804 patients underwent primary percutaneous coronary intervention of whom 24,299 (54.2%) had radial and 20,505 (45.8%) femoral access. There were 2487 (5.5%) deaths within 30 days, of which 920 (3.8%) occurred in the radial access and 1567 (7.6%) in the femoral access group. After propensity score adjustment, radial access was associated with a lower risk of death (adjusted odds ratio (OR) 0.70, 95% confidence interval (CI) 0.55-0.88, = 0.025). We found no interaction between access site and age, gender and cardiogenic shock regarding 30-day mortality. Radial access was also associated with a lower adjusted risk of bleeding (adjusted OR 0.45, 95% CI 0.25-0.79, = 0.006) and cardiogenic shock (adjusted OR 0.41, 95% CI 0.24-0.73, = 0.002).
In patients with ST-elevation myocardial infarction, primary percutaneous coronary intervention by radial access rather than femoral access was associated with an adjusted lower risk of death, bleeding and cardiogenic shock. Our findings are consistent with, and add external validity to, recent randomised trials.
本观察性研究旨在评估经皮冠状动脉介入治疗(PCI)中桡动脉入路与股动脉入路对 ST 段抬高型心肌梗死患者 30 天死亡率、院内出血和心原性休克风险的影响。
我们使用了 SWEDEHEART 注册中心的数据,纳入了 2005 年至 2016 年期间在瑞典接受直接 PCI 治疗的所有患者。我们比较了桡动脉入路和股动脉入路患者的主要终点(30 天内全因死亡),采用包含医院作为随机效应的多水平倾向评分调整逻辑回归。
研究期间,44804 例患者接受了直接 PCI,其中 24299 例(54.2%)采用桡动脉入路,20505 例(45.8%)采用股动脉入路。30 天内有 2487 例(5.5%)死亡,其中桡动脉入路组 920 例(3.8%),股动脉入路组 1567 例(7.6%)。经倾向评分调整后,桡动脉入路与较低的死亡风险相关(调整后比值比(OR)0.70,95%置信区间(CI)0.55-0.88, = 0.025)。我们没有发现入路部位与年龄、性别和心原性休克之间对 30 天死亡率有交互作用。桡动脉入路也与较低的调整后出血风险(调整后 OR 0.45,95% CI 0.25-0.79, = 0.006)和心原性休克风险(调整后 OR 0.41,95% CI 0.24-0.73, = 0.002)相关。
在 ST 段抬高型心肌梗死患者中,经皮冠状动脉介入治疗桡动脉入路而非股动脉入路与调整后死亡率、出血和心原性休克风险降低相关。我们的发现与最近的随机试验一致,并增加了其外部有效性。