Health Management Center, West China Hospital of Sichuan University, Chengdu 610041, China.
Department of Respiratory and Critical Care Medicine, West China Hospital of Sichuan University, Chengdu 610041, China.
Biosci Rep. 2020 Oct 30;40(10). doi: 10.1042/BSR20194514.
Bronchiectasis is a multidimensional lung disease characterized by bronchial dilation, chronic inflammation, and infection. The FACED (Forced expiratory volume in 1 s (FEV1), Age, Chronic colonization, Extension, and Dyspnea) score and Bronchiectasis Severity Index (BSI) are used to stratify disease risk and guide clinical practice. This meta-analysis aimed to quantify the accuracy of these two systems for predicting bronchiectasis outcomes.
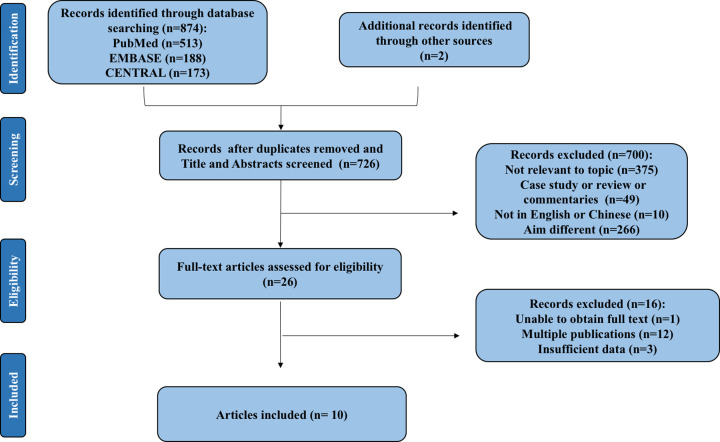
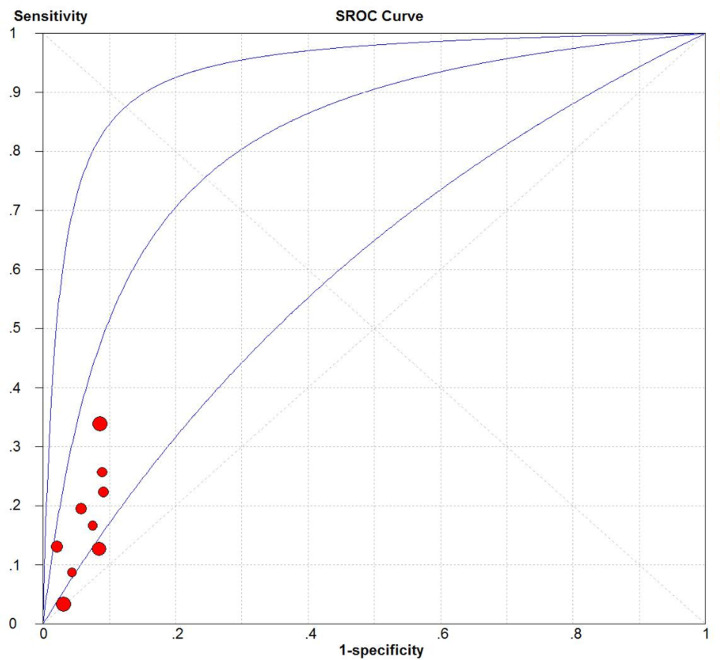
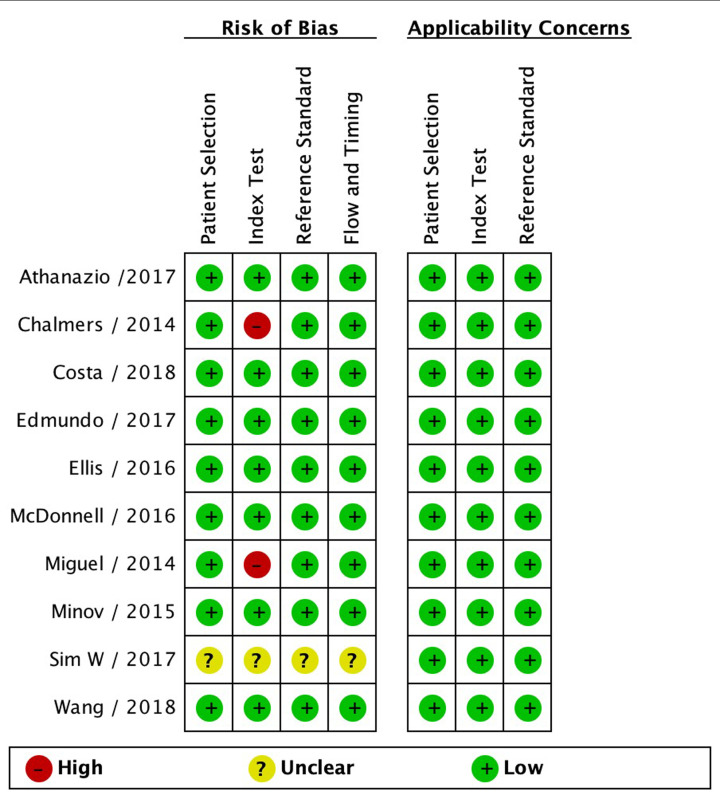
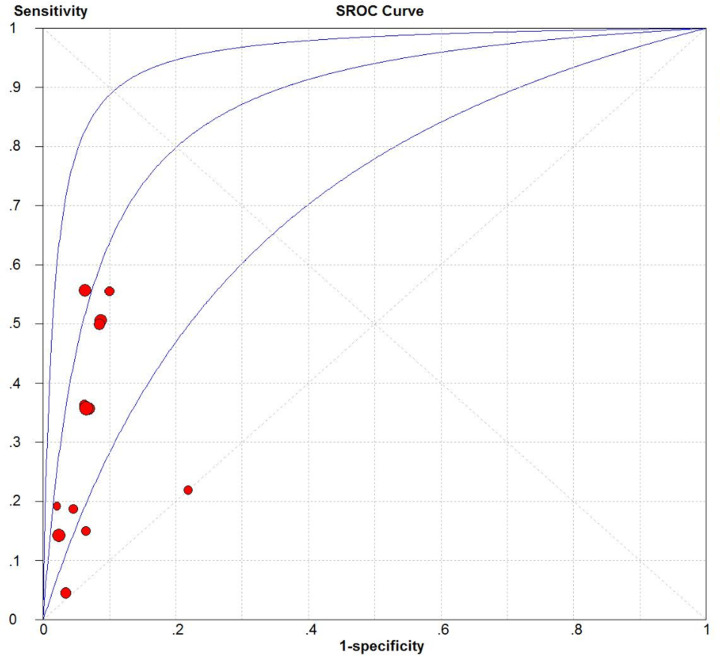
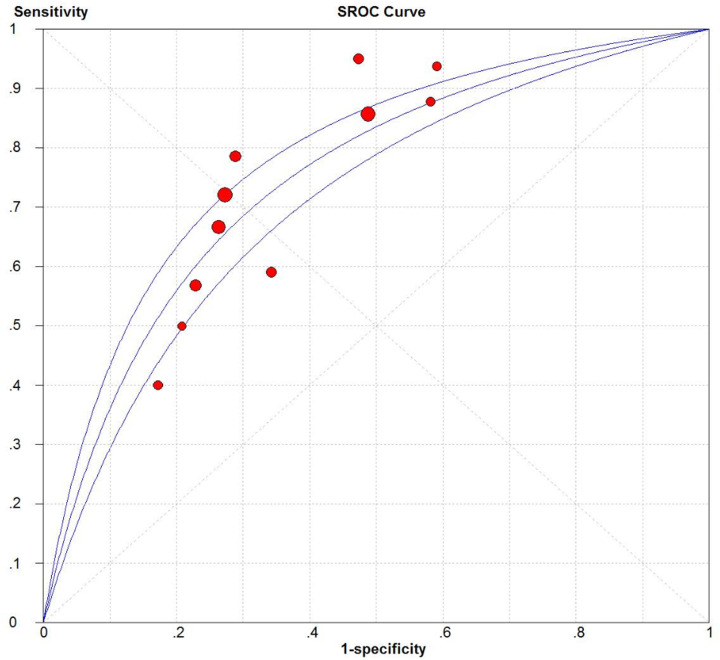
PubMed, Embase, and the Cochrane Database of Systematic Reviews were searched for relevant studies. Quality of included studies was assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) criteria. Pooled summary estimates, including sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), and diagnostic odds ratio (DOR) were calculated. Summary receiver operating characteristic curves were constructed, and the area under the curve (AUC) was used to evaluate prognostic performance.
We analyzed 17 unique cohorts (6525 participants) from ten studies. FACED scores with a cut-off value ≥ 5 predicted all-cause mortality better than BSI with a cut-off value ≥ 9, based on pooled sensitivity (0.34 vs 0.7), specificity (0.94 vs 0.66), PLR (4.76 vs 2.05), NLR (0.74 vs 0.48), DOR (6.67 vs 5.01), and AUC (0.87 vs 0.75). Both FACED scores with a cut-off value ≥ 5 (AUC = 0.82) and BSI scores with a cut-off value ≥ 5 or 9 (both AUC = 0.80) help to predict hospitalization.
At a cut-off value ≥ 5, FACED scores can reliably predict all-cause mortality and hospitalization, while BSI scores can reliably predict hospitalization with a cut-off of ≥5 or ≥9. Further studies are essential to validate the prognostic performance of these two scores.
支气管扩张症是一种多维度的肺部疾病,其特征为支气管扩张、慢性炎症和感染。FACED(第 1 秒用力呼气量(FEV1)、年龄、慢性定植、扩展和呼吸困难)评分和支气管扩张严重指数(BSI)用于分层疾病风险并指导临床实践。本荟萃分析旨在量化这两个系统预测支气管扩张症结局的准确性。
在 PubMed、Embase 和 Cochrane 系统评价数据库中检索相关研究。使用诊断准确性研究的质量评估 2(QUADAS-2)标准评估纳入研究的质量。计算汇总的敏感性、特异性、阳性似然比(PLR)、阴性似然比(NLR)和诊断比值比(DOR)等汇总估计值。绘制汇总受试者工作特征曲线,并用曲线下面积(AUC)评估预后性能。
我们分析了来自十项研究的 17 个独特队列(6525 名参与者)。基于汇总敏感性(0.34 比 0.7)、特异性(0.94 比 0.66)、PLR(4.76 比 2.05)、NLR(0.74 比 0.48)、DOR(6.67 比 5.01)和 AUC(0.87 比 0.75),FACED 评分(截断值≥5)预测全因死亡率优于 BSI 评分(截断值≥9)。FACED 评分(截断值≥5)和 BSI 评分(截断值≥5 或≥9)均有助于预测住院治疗,其 AUC 值分别为 0.82 和 0.80。
在截断值≥5 时,FACED 评分可可靠地预测全因死亡率和住院治疗,而 BSI 评分在截断值≥5 或≥9 时可可靠地预测住院治疗。需要进一步的研究来验证这两个评分的预后性能。